NBC news does a story about a teacher who had a police report filed against her because she read a book to her fifth grade students. They make it sound like this book was harmless.
“The difference is that I have that love and care for all students, not just a singular student,” she adds. “In regards to the book that was challenged in my classroom, it was a message to the LGBTQ+ community in my room and in my district that they’re ‘less than.’”
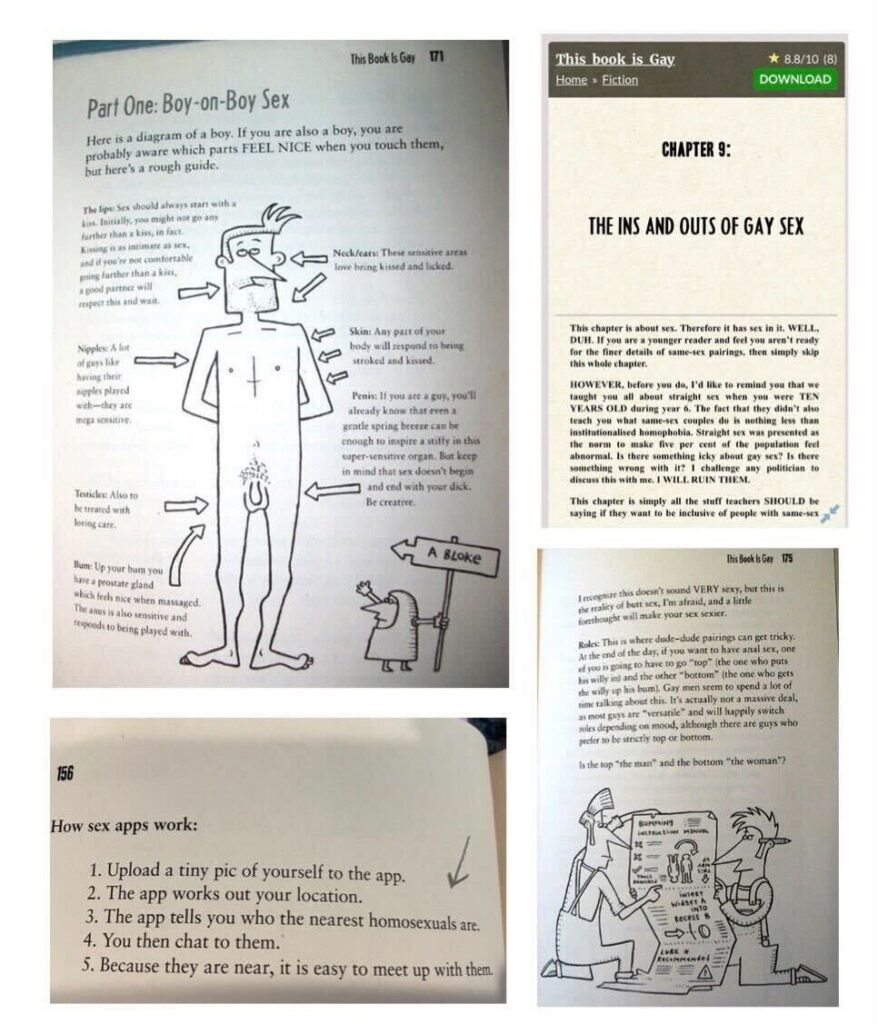
No, this book was intended to teach ten and eleven year old kids how to have gay sex. Here is some of the content of that book:
This is entirely inappropriate for children. The book claims that we teach kids about sex at ten years old. No we do not. We teach about reproduction in school, not sex. It’s done in the tenth grade for most students, the eighth grade for advanced students. I taught the class, so I know. The course is about reproduction, but makes no mention of sex. At all. We talk about sperm and egg, how they are made and how they come together to make a child. I don’t mention how the sperm gets there, nor do I give instructions on sex.
My regular carry ammo has been hard to come by for the past couple of years. I try to replenish my carry ammo every year, and I also try to standardize it across all of my carry pieces. I want high quality, effective ammo that functions well with what I carry. I buy it as if my life depends on it, because it just may. I buy it all at once, so it is the same bullet and loading.
In .45ACP: I just switched to the Speer Gold Dot G2 230gr +P. I got a good deal on it from Lucky Gunner at $27 per 20 round box. Thanks to those of you who pointed me to the Youtube video of the gelatin testing. It looks to be every bit as good as the original Gold Dot. I got a few boxes.
I still have plenty of .40S&W and .357Sig. I don’t shoot or carry them a lot, so I don’t need to buy any this year. In fact, I can’t tell you the last time I shot either caliber. That’s odd, because when I was competing in IDPA, .357Sig was my ammo. I really liked the way that it recoiled straight back and gave no real muzzle flip in the pair of black Stainless Sig229s I was competing with.
Next up: revolver ammo. I am critically low on both .38 Special and .357 Magnum. I have less than 200 rounds of each. I just don’t want to pay a dollar a round to replace it at this moment. Maybe later this summer.
One of the big downsides to having a few firearms is that you tend to accumulate various items: holsters and magazines being the two that take up the most room. I literally have hundreds of magazines in the house, all for various firearm makes and models. Some are compatible with more than one firearm. (.40S&W magazines are compatible with .357Sig, S&P 9mm magazines are compatible 9mm Compact magazines, etc.)
I was keeping the unloaded ones in large Rubber Maid totes, but looking for the magazine you need is a large pain in the, well Rubber Maid tote. So I began looking for an answer, and it didn’t take me long to find one. I bought some foam rubber holders that fit into a .50cal ammo canfor handgun magazines . I decided to try them out. Four of them cost me $62.
You number your mags too, right?
These holders allow you to store 24 magazines in each ammo can. That means I can have a can with just Smith and Wesson full sized 9mm magazines, another with .40 and .357 magazines, etc. Now four ammo cans take up the same amount of room as one Rubber Maid tote, and hold 96 magazines in a way that makes it easy to find the one you are looking for. The cans that I have are lockable, so that allows me an extra layer of security.
The downside is that the things aren’t as rugged as I would like, and lots of use will probably tear them up. Still, it’s better than what I had. If I didn’t already have the cans, I would look at buying cans that come with the pluck n’ pick foam already in them. It’s cheaper that way.
Now I need some storage for rifle magazines and for the large number of holsters that are sitting around here.
Now, the disclaimer: I don’t advertise, and receive nothing for my reviews or articles. I have no relationship with any products, companies, or vendors that I review here, other than being a customer. If I ever *DO* have a financial interest, I will disclose it. Otherwise, I pay what you would pay. No discounts or other incentives here. I only post these things because I think that my readers would be interested.
Apparently, they only did it as a symbolic gesture, fully intending that the illegals stay down there in the south, where the unwashed hicks live. They are now protesting against the illegals being kept in their kids’ school. Note that most of the protesters are not white. Huh.
If it wasn’t for double standards, leftists would have no standards at all.
Today’s video comes from Charleston County, South Carolina. On May 7, Deputies Evan Cubbage and Alexander Hodge conducted a traffic stop on a black Crown Victoria. They had an ordinary interaction with the driver and passenger for just under seven minutes before asking the passenger to step out of the car. That’s when things went sideways:
A year ago, I reported on an incident at a Target where a group of “teens” were stealing from a Target store. The store contacted police, who just happened to be conducting training nearby, and the cops attempted to take the young criminals into custody. The criminals, who were illegally armed with at least one firearm, tried to ram the responding deputies, whereupon the cops fired multiple shots into the car, killing one and wounding two others.
The reason I mention this is because the criminals are now suing Target for the cops shooting them, claiming that Target allowing the cops to use their parking lot for training was some sort of conspiracy to use the criminals as training subjects, so the police could use vehicles and guns on live subjects.
One of the claims is that Target knew, through their video surveillance, that the three thugs were stealing. They also knew that the cops were outside. The lawsuit claims that Target has a duty to warn all of its customers of hazards that may be present on the premises, and therefore has a duty to warn shoplifters that the cops are outside waiting to arrest them.
This is the kind of thing that lawyers should be penalized for doing. Our courts are overworked as it is, and this is the kind of money hunting, ambulance chasing behavior that needs to be discouraged. There are plenty of companies out there that are total jerks and need to be dragged into court. This case isn’t one of those.
The money is gone. They spent it. Like a dad who is angry because when you sent your kid off to college, you gave him your credit cards to use in the event of an emergency, and he maxed them all out on unnecessary bullshit, it’s our fault for giving them essentially unmonitored access to the credit cards. Yep, I said it- it is our fault for not watching what they were spending the money on. So now we have $200,000 in maxed out credit cards, and nothing to show for it. Except in this case, it’s $35 trillion worth of useless treasury notes, and a bunch of promises.
So yeah, everyone is getting screwed. Take a moment to let that sink in. Now feel the anger? You pissed off? Well, so was I, when I first began to realize just how fucked we are.
The time to complain about that was when the Congress spent DECADES throwing money around like a Frat boy with his dad’s credit cards. And yes, it was spent on bullshit.
$190,000 by Senator Charles Schumer (D-N.Y.) for digitization of the New York Historical Society’s photo collection.
$200,000 by Rep. Howard Berman (D-Calif.) for the Providence Holy Cross Foundation tattoo removal violence prevention program in Mission Hills.
More than $220 million to build a bridge between Gravina Island, an island that was home to 50 residents at the time, and the Ketchikan Airport.
Don’t think that the holy grail of the Republicans, the defense budget, was immune from this waste. Rep. Duke Cunningham (R-Ca.) resigned and pleaded guilty to accepting $2.4 million in kickbacks from military contractors for steering billions of dollars worth of defense budget dollars their way, using his positions on the Defense Appropriations subcommittee and the Intelligence Committee to insert earmarks for military spending.
$500,000 in federal funding for the construction of a very unique museum in Sparta—a town that had a population of about 18,000—the Sparta Teapot Museum of Craft and Design.
$14.8 billion to Boston for a tunnel (The Big Dig) that was the most expensive highway project in history.
$3.4 million for a tunnel in Florida that would allow turtles to cross Highway 27 safely.
Decades of wasteful project after wasteful project, adding up to hundreds of trillions of dollars in spending. Every single President since Eisenhower has been a part of it. Who is blame? We are. We let them do it. Let the anger soak through you, then take a deep breath. Let it out. I agree with you. It sucks.
The money is gone. There is no way that it will ever be paid back. We owe more money than physically exists. That right- add up all of the money in the world: Dollars, Euros, Yen, Yuan, all of it. Now send it all in. That doesn’t even pay what the US owes, much less the debt of all of the other nations in the world. Now you begin to see just how fucked we all are. Yes, I am using the word “fucked” even though profanity is not used here very often. Why? Because no other word really begins to describe just how bad things really are.
There is no way out of this. The bill is going to come due, and we are the ones who will be stuck with it. That pension you are owed? Gone. The Social Security fund that took from you a third of every dollar that you earned for your entire working life? It’s been spent. I’ve been warning you about this since I figured it out, back in 2007.
Again, the time for us to have fixed this passed some time ago. I became an adult during the Reagan administration. It was probably already too late at that point. My generation inherited the problem, but we certainly didn’t even try to fix it. So yeah, I blame the Boomers (and my own parents, who were part of the silent generation) for creating the problem, but the generations since then certainly didn’t try to fix anything. That makes all of us responsible.
Lacta alea est. It’s too late to cry over spilt milk. You can be mad, but that is like the old man yelling at clouds: it doesn’t change anything.
All we can do now is try and save what we can, and in my opinion, all we can do is try and save our local area. Be ready, band together with as many like minded neighbors as you can, and try to weather the storm. Sauve qui peut.
Get skills. Stockpile tools, gear, food. Learn to garden. Plan. Make friends with neighbors who have complimentary skills. Stockpile stuff that you can trade to people with skills who may compliment your own. For example, extra guns for neighbors who may not have one. They can use it to stand watch while you sleep, or cover your backside.
It’s coming. We don’t know when, but at this point, it’s undeniable.