The next time someone tells you how another country’s health care is better because it’s free, show them this.
He called EMS at 1755, again at 1805, complaing of shortness of breath. He was told no ambulance would be coming, but that a doctor would call him back.
Someone finally called at 1907, but no one answered that call or tow others. An ambulance was finally sent at 2112,arriving at 2119.
The man was dead on the floor. Hey, at least it was free.
Very enlightening. Up to now, I assumed it was big pharma and greedy insurance companies that caused health care costs to skyrocket. The correct answer, as it turns out, is all of the above; everything connected to healthcare.
No offence to oldvet, this post isn’t an attack upon him, but is a classic case of supply and demand. The ED wants to open, but there is a shortage of qualified nurses. They have no choice if they want to stay in business- by law, an emergency room has to be open 24/7. So they have to:
do whatever it takes to get qualified people to come in: that means paying enough to entice them or
lower standards and risk medical errors
Since the US has a climate of legal liability, medical care is a field that has zero room for errors. People who can treat patients without making a single error are rare and in high demand. That means there is a bidding war for their time.
Skilled people cost money, which is why it costs $165 to have a plumber snake a drain. No one wants to look up while having a medical emergency and see the cheapest nurse caring for them- they want the best, or at least someone who is good at what they do.
It takes 3-4 years to train a basic nurse. More than 3/4 of those who begin the education don’t make it.
Then it takes another year to train for the ED specialty. Two more years before they reach a point of proficiency without needing guidance and supervision.
Of the nurses here who manage that seven year slog, just over ten percent are good enough to be board certified in emergency medicine. Only a quarter of those have two board certifications.
In other words, of the 257,000 actively licensed RNs in Florida, 17,000 are Emergency Room nurses. Of ED nurses, only about 2500 of them are board certified. Only about 800 of them have two certifications.
Are two specialties really needed? Certified Emergency Nurse, sure. How about a nurse certified in stroke care? Pediatrics? Trauma? Vascular access? Critical care? Each of those is a subspecialty that is needed in the ED on a daily basis.
Now consider that there are 477 licensed emergency departments in Florida, all competing for those nurses. Everyone wants the best, so those who have multiple certificates and degrees demand (and get) top dollar. My last employer had 162 ED nurses and still didnt have enough for their patient load. That drives up costs.
They only way to eliminate the nursing shortage is to either lower demand or increase supply. Lowering demand isn’t going to happen. Raising supply can be done in two ways:
Raise pay
Lower standards
In today’s legal climate, lowering standards would actually cost more in increased litigation caused by more medical errors. In the ED, 95% of patient care is performed by nurses. We write orders for imaging, lab work, and treatment. What kind of provider do YOU want at your side during your next medical emergency?
This is a story of a patient from a year or so ago, while I still worked for my last employer.
A patient comes in because he has had increasing shortness of breath for about two weeks. He was walking down a small hill from where he parked his motorcycle and fell, tumbling down the small incline. He fell about 10 feet or so, he says. His vitals look fine. He is a bit of an overweight guy, typical 60-something man trying to recapture his youth by riding a Harley.
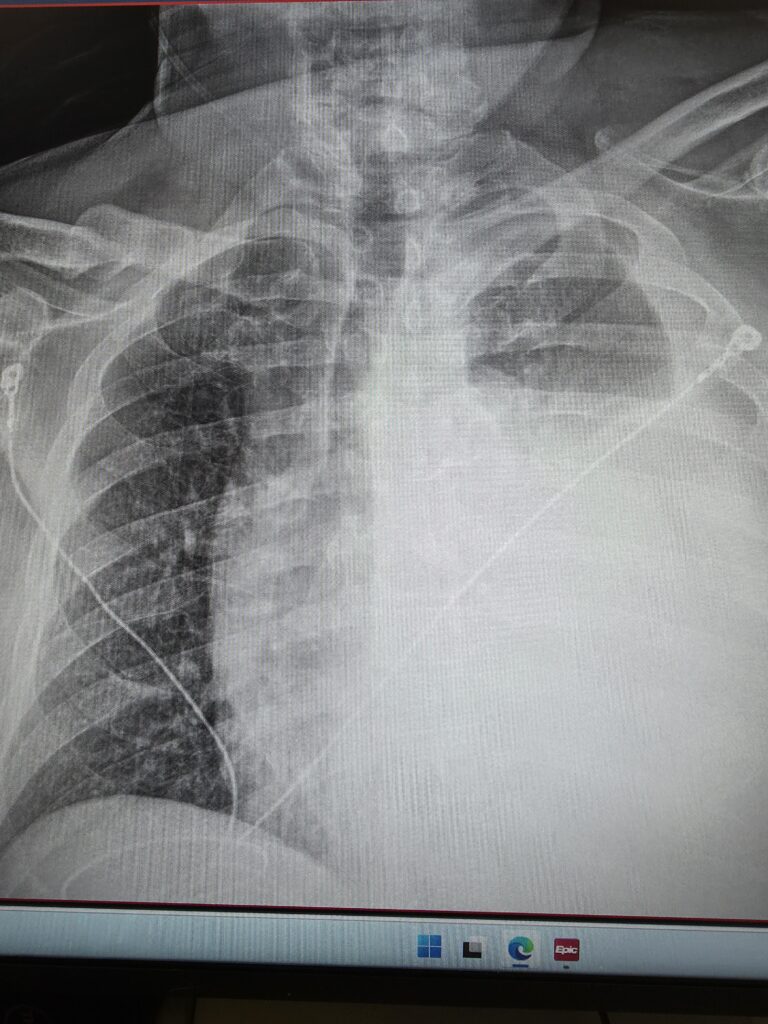
So I ordered a chest x-ray, started an IV, and did his intake paperwork. No doctor is signed on to his case yet. If the x-ray shows anything significant, the technician who takes it will normally give me a heads up. He didn’t in this case. The image of the x-ray came up on my computer, I took one look at it and immediately flagged down the first passing doctor and said, “Hey, I know that you’re busy and this isn’t your patient, but you need to see this now.” Here is what it looked like:
In case you don’t know what you are looking at, the dark section on the left is a relatively normal looking lung. The heart and trachea are supposed to be on the right side of the image and are being pushed into the other side by the large amount of blood that is collapsing his left lung (which appears on the right in this image). If you look closely at the film, you can see all of the structures that are supposed to be midline are being pushed over. This is called a hemothorax, and is a life-threatening medical emergency where a massive volume of blood rapidly accumulates in the pleural space (the area between the chest wall and the lung). This buildup compresses the lung and puts dangerous pressure on the main vein bringing blood to the heart (the vena cava) and the heart, leading to cardiovascular collapse, severe respiratory distress, and shock.
The doctor took one look at this and said “Holy shit! I’m signing up for him. Get me set up for a chest tube and some conscious sedation. Call respiratory and let’s get ready to send him to a trauma center.”
The patient had a rather chubby neck with a beard so it wasn’t readily apparent, but if you put the finger of one hand on his Adam’s apple, and a finger from the other hand in his sternal notch, you could see that his windpipe was deviating to the patient’s right. He was a good sport and didn’t even mind that I brought a couple of new nurses into the room to see what a tension hemothorax looked like. Of course, he had no lung sounds on the left, and his heart tones were distinctly muffled. His pulse pressure was a bit narrow.
There were not any other nurses or respiratory technicians available to help in time, so I grabbed a nursing assistant and the three of us (doctor, myself, and aide) rapidly initiated conscious sedation and inserted a chest tube. That’s a handful for one nurse and a doctor to handle (the nurses aid is pretty much there to hold this, and hand me that and isn’t much of a help)- I had to administer sedation, monitor and maintain his airway and breathing, and chart everything. For one nurse to do all of that without help is a major safety issue, and is one of the (many) reasons why I don’t work for that hospital any longer. That place is just understaffed to the point of compromising patient safety.
Once we got the tube in place, we sent him for a CT scan, and it turns out he had 4 ribs broken in two places- a classic flail chest. If you put your hands on his rib cage, you could feel the paradoxical motion of the chest wall. This is incredible, considering that he walked in to the ED and had been walking around like this for two weeks. The video below shows you what paradoxical motion looks like, but my patient’s wasn’t quite as pronounced as the video (and was located under his left armpit).
Anyhow, I pulled about 2 liters of blood from his chest cavity before we crimped off the tube because we didn’t want him losing too much blood. A helicopter came and took him to a trauma center, and the trauma surgeon was still pissed because we took out so much blood.
A few of my readers have commented on how they enjoy practice pearls, so I thought I would go ahead and share a simple one. This particular pearl is not just for medical people, it will work quite well for those of you who are not in the medical profession. In the medical profession, a lot of time is spent training people in the latest, greatest technology- the newest medication, the latest technique, the wow factor, but sometimes, it is the old school method that works best. I recently had the chance to teach a young doctor this exact lesson.
Lacerations
We had a woman that entered the emergency room who had cut off the last quarter inch or so of the tip of her finger with a pair of scissors while attempting to cut open an Amazon package, of all things. In so doing, she had also managed to nick the artery, and blood was pulsing out of the end of her finger. She had the presence of mind to bring in what she thought was the tip of the finger (what she brought in wasn’t the finger) and she was attempting to control the bleeding herself, but wasn’t succeeding.
The doctor looked at it and suggested we perform a digital block and attempt to stitch off the artery and suture the wound closed. That was going to be a bear to do. Instead, I suggested that we try something a bit more old school. I took a large emesis basin, filled it with ice, a little water water, and a bottle of Providone. I told the woman to place her finger in the basin and keep it there until the cold became painful. This concoction does three things:
The ice numbs the area
the Providone cleans the wound (there is a risk of infection if you don’t)
the ice also constricts blood vessels and is great at controlling bleeding
She spent about 15 minutes with her hand in that basin, and this stopped about 80% of the bleeding. I pulled her hand out, cleaned the finger with a couple of gauze pads (4×4), then had her hold one against the tip of her finger using her thumb. After about 5 minutes of that, we still had some bleeding, so I soaked a gauze pad with tranexamic acid (TXA) and placed it against the wound. That stopped the rest of the bleeding. I dressed the wound, and we sent her home.
Esophageal Varices
Just as you can get varicose veins in your legs, you can get them in your esophagus as a result of cirrhosis of the liver and the resulting portal hypertension. I was working in the ED one night when a patient began vomiting large amounts of blood. I’m not talking about what most people would think are large amounts of blood, but what a nurse who works in the ED thinks are large amounts of blood. It looked like this:
We were under the gun: if this bleeding didn’t stop, we were looking at a dead patient. I inserted an NG tube to suction out the blood, and the doctor and I came up with a plan. Using a piston syringe, I would push about 100 ml of ice water into the tube, let it sit for about 30 seconds, then suction it back out. I repeated this about 5 or 6 times, and each time, the amount of blood that came out with it was less. I was forced to stop after that 5th or 6th time, because the cold must have been irritating to her heart, as evidenced by the fact that she began having short runs of ventricular tachycardia. For that reason, anyone trying this, I would recommend placing the patient on a cardiac monitor and keeping a close eye on on their heart rhythm while doing this.
Ice- it’s quite useful in emergency medicine, but it isn’t used much any more in emergency medicine because it doesn’t have the sexy feel of the latest, greatest advances in medical technology, but it is still damned effective. Sometimes old school is still the best way to go.
Imagine Congress passes the “There Is Such a Thing as a Free Lunch Act” (TISFATLA). The law is simple and well-intentioned: No American should go hungry during the workday. Therefore, any restaurant that chooses to remain open between 10:30 a.m. and 3:00 p.m. must provide a nutritious lunch, defined as at least 500 calories of balanced food (protein, vegetables, whole grains, etc.) to anyone who walks in and requests it, without regard to their ability to pay, insurance status, or how many times they’ve eaten there that week.
Restaurants aren’t completely cornered. They can still raise prices on breakfast and dinner, seek government subsidies, reduce portion sizes, shorten hours, or even close during lunch. But they must serve first and ask questions later, or face steep fines (tens of thousands of dollars per violation) and possible loss of their operating license.
What Happens Next?
Immediate effects: Lines snake around the block. Demand surges because the price at the point of service is zero. Office workers, students, tourists, and predictably frequent diners treat the restaurant as their new daily cafeteria. A tiny fraction of “super-users” (maybe 1–2% of customers) begin consuming 10% or more of all free lunches. One motivated individual might rack up 20–30 meals a month. Why stop? It’s “free.”
Restaurants respond as any business would: they raise breakfast and dinner prices sharply to cover losses, cut quality, shrink portions, and reduce staff. Some simply stop serving lunch altogether, shrinking overall supply and making the remaining spots even more crowded. Wait times balloon to an hour or more. Working people who can’t stand in line during their short break go hungry—not because they lack money, but because the queue rations access.
The Government’s “Solution”: More Rules
Instead of admitting the law created perverse incentives, policymakers declare the problem is “greedy restaurants” exploiting loopholes. So Congress and regulators respond with layer after layer of new rules to “fix” the distortions:
Restaurants must now document every free lunch with detailed nutritional logs, customer affidavits of need, and proof that the meal met exact caloric and macronutrient guidelines.
They have to submit monthly reports to a new federal “Lunch Equity Commission” showing how many free meals were served, to whom, and at what cost.
To prevent “abuse,” restaurants must implement a national “Lunch Eligibility Verification System” that cross-checks customers against a government database— but they still must serve first and verify later.
New mandates require “culturally appropriate” options, allergy accommodations, and sustainability standards for ingredients.
Complying with this exploding regulatory thicket isn’t cheap. Restaurants now have to hire entire new departments of billing specialists, compliance officers, nutrition auditors, and paperwork clerks just to navigate the rules and avoid ruinous fines. These added administrative costs get passed on through even higher dinner prices, smaller portions, or reduced service quality. Some smaller restaurants simply give up and close.
The result? The original promise of “free lunch” has morphed into a vast, expensive bureaucracy that employs more people pushing paper than actually cooking food. Meanwhile, lunch lines remain long, quality has declined, dinner prices have skyrocketed, and fewer restaurants are willing to stay open during the mandated hours. Everyone begins complaining that the nation’s “restaurant system” is broken. Why, in Europe, people just walk in and buy lunch without waiting!
The EMTALA Parallel Is Striking
This cycle is not hypothetical, it’s exactly how EMTALA and the broader healthcare regulatory regime have evolved. A hospital shows up with a possible emergency? Screen and stabilize first, payment questions later. When uncompensated care piles up and emergency departments become overcrowded with frequent flyers (a small group of patients driving a wildly disproportionate share of visits and ambulance runs), the response isn’t to revisit the zero-price mandate. Instead, we get more rules: ever-stricter documentation, quality metrics, electronic health record mandates, billing codes, prior authorizations, and compliance layers.
Hospitals and physician groups respond by hiring armies of coders, billers, compliance staff, and administrators. U.S. healthcare now spends roughly 25–30% of total dollars on administrative overhead — far more than in most other countries. That bureaucracy doesn’t deliver care; it manages the distortions created by mandates, price controls, and third-party payment systems. The original goal of helping people in genuine need gets buried under mountains of paperwork, while costs keep rising and access problems (long waits, boarded patients, specialist shortages) persist.
The Deeper Lesson
When someone tries to use jury duty, court-appointed lawyers, or judges as justification for forcing doctors and hospitals to provide “free” healthcare, they’re missing (or ignoring) this dynamic. The justice system obligations are narrow constitutional protections against government abuse of its own punitive power. EMTALA-style mandates in medicine are open-ended entitlements that conscript private resources and then breed ever-more-complex regulation to manage the inevitable shortages and abuses.
There is no free lunch, just as there is no free healthcare. Every attempt to create one through mandates simply shifts the costs (to paying customers, taxpayers, or future patients) and grows a parasitic administrative class that feeds on the resulting complexity. The compassionate impulse to help the needy is better served by increasing real supply: more doctors, fewer barriers to entry, price transparency, and targeted aid, rather than layering on rules that make the system slower, more expensive, and less responsive to actual human needs.
The problem is one of intelligence. How do you create more doctors, nurses, and other medical personnel without lowering standards? Medicine (and advanced nursing) is cognitively demanding. It requires high fluid intelligence, strong working memory, pattern recognition, and the ability to integrate massive amounts of complex information under pressure. Multiple studies put the average IQ of physicians around 120–130 (roughly the 90th–98th percentile of the population). That’s not an accident or a gatekeeping artifact; it’s what the work demands. You can’t mass-produce doctors the way you can produce more Uber drivers or retail workers without either lowering standards or hitting the natural limits of the talent pool. There are ways to increase the number of health care workers, and we can discuss that in a later post.
In case you are wondering, this post was written because of this guy:
People are guaranteed a right to an attorney if charged with a crime. That's another man's labor.
The left loves to tell everyone how the US needs to have “free” healthcare, you know, like they do in Canada. Let me illustrate why that’s bull hockey.
I was at work, and a man brought his 17 year old son in, after the son fell off of his dirt bike a week before, injuring his shoulder. X-ray showed no broken bones. The dad asked if we could see any tendon or muscle damage, and we informed him that an x-ray can’t see that, he would need more testing. At this point, it is no longer in the scope of emergency care. The doctor and I advised them they would need to go to the child’s doctor’s office to get an order for an MRI, because only an MRI could see with that kind of detail.
The dad then asked if we could write the order for the MRI. The doctor explained that ER doctors can’t write an order like that, because the doctor writing an order for tests has to be the same doctor who treats the patient’s conditions exposed by that test. The man explained that the child’s doctor wanted him to have an MRI. So we asked him why he doesn’t get his own doctor to write the order. Even if insurance won’t pay for it, it’s only about $200.
We are from Canada and are returning home in the next couple of days. I can’t believe you won’t just give me an order. This is ridiculous, not only do we have to pay almost $300 for this ER visit, you can’t even write us the order to get the MRI. Now you want us to pay for a local doctor and pay $200 for an MRI? The health care system here in the US is so broken.
We asked, “If you can get it done for free back home, then why don’t you get it done when you get there?” His reply was gold:
We specifically came here to the US get an MRI because there is a year long wait for one back home. We tried to get one at the place down the street, but the MRI place said we need a doctor’s order. All I need is an order from a US doctor so we can get one while we are here in the states.
That’s the state of Canadian healthcare. It’s free, but you can’t have any. Rather than wait, this dad bundles his kid up, flies to the US, then trashes our medical care because it won’t do it now, and won’t do it for free.
Nursing is a great job because it’s a large tent. There are jobs for nurses both in and out of hospitals. I can’t speak for out of hospital nursing because I don’t have any experience whatsoever, but in hospital there is a hierarchy, and it’s the same in nearly every hospital, to the point that memes are made about this.
Nursing has a definite pecking order. Let me say that each nursing specialty is needed, but some nurses do have a more strenuous pathway than others. Remember that nursing is filled with mostly women (about 65% female) and women are some catty, backstabbing bitches. It makes for some very cat-like behavior, and not in a good way. No, in a “mean girls” way. The bullying and competition is pretty fierce. Women are simply vindictive, conniving bitches.
You have your inpatient nursing- medical/surgical (called med-surge), and these nurses staff the oberservation and general patient floors. Generally, med-surge nurses care for the least complicated patients, and they tend to be the least skilled nurses in the hospital. I’m sure that will piss some people off, but that’s just how it is. Because the patients are low acuity, nurse/patient ratios are 1:6 or sometimes as high as 1:8.
A step up from that is cardiology, oncology, wound care, those sorts of specialties. Nurses in these areas are very good within their specialty, but don’t generally know a whole lot outside of it. Again, they are needed, and a great example is that I suck at wound care, so not slamming anyone. The nurses in this area are usually ratioed at 1:4 or 1:5.
Above the general floor nurses are your step down units- PCU, CVPCU, those kinds of units. These nurses handle patients that are more complicated and require more care. For that reason, ratios are usually 1:3 or 1:4.
The next level up in the inpatient nurses packing order is the ICU. The nurses in this unit generally consider themselves to be the cream of the crop. There is a bit of a superiority complex here, and a good bit of it is well deserved. ICU nurses are well known for being very detail oriented and for having OCD. Every IV line is carefully labeled with color coded stickers. The ICU nurse knows everything there is to know about the patient: the name of his kids, his dog, his favorite color. They have time for that, because the nurse patient ratios are frequently 1:1 or 1:2, so they spend the entire 36 hour workweek with 1 or 2 patients.
Then there are outpatient nurses. PACU (post anesthesia care unit) nurses take care of patients who have just come out of surgery. After that the patient either gets admitted to an inpatient unit, or goes home. Also surgical nurses, endoscopy nurses, and the like. The nurses here are fairly specialized, and most of them work M-F 9-5 jobs. Other nurses refer to these types as “princess” and the shifts they work are called “princess shifts.”
The emergency department. The nurses here are known as being “cowboys” who don’t follow the rigid rules the rest of the hospital’s nurses have to follow. They have one overriding goal- stabilize a patient, then send them to an inpatient unit. Everything else- bathing the patient, changing their clothes, and other nursing tasks just don’t get done. ED nurses also tend to think of themselves as being the best of the best, and act like those routine tasks are beneath them. For this reason, inpatient nurses generally don’t like ED nurses.
If anything goes wrong in an inpatient nurse’s area, the nurse will initiate a “rapid response” or “CAT” call, and the response team will come to help them out. Some hospitals use ICU nurses as the response team, other hospitals use ED nurses.
As you can imagine, the rivalry between ICU and ED nurses can be rather intense, med-surge nurses feel (or are looked down upon) as being inferior, and the entire hospital feels like it is at war with one unit, shift, or zone being at war with all of the others. Some temporary alliances are formed, mostly when one unit teams up with another to take a third unit down a peg or two.
Yes, nursing is filled with a bunch of infighting that is mostly caused by having several hundred women in the same building, all wearing the same outfit, and about 1 in 5 of them is menstruating at any given time. It’s like being in a building full of rabid honey badgers.
All shift long, it’s “day shift is lazy,” or “Night shift didn’t do anything last night,” then you hear “Med-surge nurses are idiots,” or “Those ICU nurses are stuck up bitches,” and the old reliable “The ED nurses didn’t even bathe this patient and put him in a gown before they sent him up.”
Older nurses take great pleasure in screwing with younger ones, for no other reason than flexing their pecking order muscles. It’s so bad that every nurse hears an old adage while they are in school: “Nurses eat their young,” meaning that the level of bullying of new nurses by old ones sends many a young nurse off to cry in the bathroom.
It’s especially difficult when you are a man that just doesn’t like playing those kinds of bullshit power struggle games, and also has the nasty habit of calling things like you see them. It’s been a difficult skill to learn, biting my tongue. I still struggle with it frequently. I’m old enough that I don’t play those games, and I tell people to fuck off. That’s when your attacker then plays the victim card and uses their victim status as a weapon.
My first experience with this was in nursing school, when a fellow student began bitching at me and calling me stupid, and I told her to shut the fuck up. I almost got kicked out of school after she went to the instructors and told them I was racist and sexist. For the rest of school, that woman (who also happened to be black) organized a “Hate on Divemedic” club amongst the other students and staff members of her own demographic.
If you get the feeling that I don’t like most women in the workplace, you would be correct. They spend more time setting up tribes, posturing, backstabbing, and putting on makeup than they do actually caring for patients. There is a lot less of that kind of bullshit in the ED, simply because we are too busy to have time for that shit. Let there be some down time, and the ED starts with it too.
It’s exhausting.
I got a message from a reader who is a nurse, talking about my last work post. The gist of it was “be careful making enemies of HR and training folks, they will screw you over.” You know what, that is 100% correct, nurses like that will find a way to get back at you. The difference now is that I am close enough to retirement that I just don’t care.
This is for my medical readers, a little pearl from critical care in the ED. This was a case I recently had in my care. Look at what decision making goes into critical care:
A patient presents with acute severe dyspnea consistent with hypertensive acute decompensated heart failure (flash pulmonary edema).
Initial Assessment:
Respiratory:RR 40/min with sternal retractions. Severe air hunger despite NIV. EtCO₂ 31 mmHg (hyperventilation, not ventilatory failure). SpO₂ 100% on NIV. Cardiovascular:HR 120 bpm BP 218/184 mmHg (marked sympathetic surge / afterload crisis)
Clinical interpretation:The patient was not hypoxic and not retaining CO₂, but was in extreme sympathetic overdrive with excessive work of breathing and anxiety worsening pulmonary congestion.
Intervention
Continued noninvasive ventilation (NIV). Morphine 2 mg IV administered as a targeted adjunct for refractory air hunger and anxiety. Reassessment (15 minutes post-administration)
HR: 95 bpm RR: 18/min BP: 142/72 mmHg SpO₂: 96% (clinically acceptable). Work of breathing markedly improved; patient calmer and tolerating NIV.
Teaching Points
Air hunger in acute heart failure is often driven by pulmonary congestion and sympathetic activation, not hypoxia alone. EtCO₂ of 31 mmHg confirms hyperventilation and preserved ventilatory reserve, reducing concern for opioid-induced CO₂ retention. Low-dose morphine (2 mg IV) in this setting blunts excessive catecholamine response, reduces central perception of dyspnea and panic. It produces mild venodilation, which lowers preload/afterload, and improves tolerance of NIV without suppressing respiratory drive.
Why this was appropriate: Although the use of morphine in heart failure is an old therapy that has been largely discredited in modern studies, it was appropriate in this case. NIV was already in place (airway support maintained), continuous monitoring, including EtCO₂, was available. The dose was anxiolytic, not sedating, and the primary threat was sympathetic storm, not respiratory failure.
Key Teaching Pearl
Morphine does not treat heart failure and can actually be harmful in many cases, but in rare, carefully selected patients, low-dose morphine can interrupt a life-threatening sympathetic–dyspnea feedback loop when NIV alone is insufficient.
Practice Implications
Morphine should not be routine in acute heart failure, consider only when:
Severe air hunger persists despite NIVEtCO₂, which indicates hyperventilation (not CO₂ retention)
Blood pressure and monitoring allow safe administration
Always pair with definitive therapy (NIV, BP control, diuresis)
My charge nurse disagreed, saying all HF should be treated with nitroglycerine and loop diuretics. That’s simply blind protocol adherence. The doctor and I disagreed with that, to the patient’s benefit.
Bottom Line
This case illustrates that physiology-guided, low-dose morphine when used judiciously and with monitoring can be a safe and effective adjunct for refractory air hunger in hypertensive acute heart failure, reinforcing the importance of individualized clinical judgment over reflexive protocol avoidance.
In a move that signals just how much of a fascist tyrant he is, Trump signed an executive order reclassifying marijuana from Schedule I to Schedule III on Thursday. Schedule III drugs are things like Ketamine, Testosterone, and Codeine. That sets in motion a number of things that are important. The most obvious of these is that users of medical marijuana are no longer unlawful users of the drug, which also means that those with a medical marijuana card are no longer prohibited from buying a firearm, and can now legally put no on a 4473. It also means that BATFEIEIO will have to revise and rewrite their form 4473 questions.
Republicans are incensed because police unions have long opposed such a move, as busting people for weed is a huge source of police employment and a great way to conduct warrantless searches: “I smelled weed.” As evidence to support their ire, Republicans made the following points:
Reclassifying marijuana as a Schedule III drug will send the wrong message to America’s children, enable drug cartels, and make our roads more dangerous
According to a recently published fifteen-year review of medical research, marijuana has no real medical value, and 30% of medical marijuana users have an addiction to the drug
Under Schedule III, pilots, truck drivers, and other safety-sensitive professions will not be tested for marijuana.
Marijuana is already imperiling safety: over 40% of fatal car crashes today involve THC. Rescheduling will exponentially worsen this crisis
First, let me say that I am one of the only people that I know that has never even tried the stuff. I have no interest in it, and I just never felt the need to try it. My only oppositions to marijuana are practical ones.
I hate the smell when it is smoked. It reeks. I don’t care if they legalize it, as long as I don’t have to smell it. Make it an edible, or make patches. Do that, and I won’t care.
Pass limits beyond which someone is considered impaired, and come up with a test that can reliably determine if someone is beyond that limit. I don’t want someone flying my plane or surgeons operating on people while they are impaired.
Now that that is out of the way, let’s address the Republican claims:
America’s children aren’t sitting there saying “Oooh, Trump said doctors can now prescribe weed. I think I will go out and smoke it now.” Ridiculous. Anyone who wants weed gets it now. I know that it’s anecdotal, but I would say that half of the people under the age of 30 who come to the ED test positive for marijuana, and probably 1 in 5 who are over 30 do as well. The patients I don’t test smell like weed a good bit of the time, too. Your policies aren’t doing shit to prevent people from using.
Half of the states (almost- it’s 24 now) have already legalized marijuana in some form or another. The Federal government is just catching up with what the states are doing, and what the citizens obviously want.
Marijuana DOES have medical uses. The fact that studies are showing that it doesn’t is a reflection of science being for sale. The government pays someone to conduct a study on marijuana to prove it has no legitimate use, and what do you know, the preexisting opinion of the study’s sponsor is confirmed. Far too much of what we call “science” is actually paid propaganda. Most “scientists” are actually whores who sell the weight of their credentials to the highest bidder.
Truck drivers, pilots, and the like can still be tested for weed as a Schedule III drug. They are tested for intoxication on things like alcohol (no scheduled at all), Schedule IV drugs like Xanax, Ativan, and Valium, as well as other Schedule III drugs like Ketamine and Codeine. This is just a stupid and downright untruthful argument that I classify as fear mongering, no different than “every traffic accident will result in a gunfight.”
In my several decades as a paramedic, I can say that nearly every traffic accident occurring after midnight involves an alcohol impaired driver, and we aren’t making alcohol illegal. If fatal accidents involve a driver with marijuana in their system 40% of the time, I ask how many people have marijuana in their systems. Correlation doesn’t imply causation. I could easily say that 60% of people who die in a traffic crash eat sandwiches, but that doesn’t make sandwiches the cause of traffic deaths. Keep in mind that current testing for marijuana doesn’t test for intoxication, it tests for presence. Because they are fat soluble, the metabolites of marijuana stay in your system for up to 90 days. That doesn’t mean that you were intoxicated at the time you were tested, which is my second point, above.
Overall, I think this issue is a loser for Republicans, and I support the action Trump took here. I just wish I didn’t have to smell that stuff everywhere I go.
Just as many so-called “conspiracy theorists” have been telling us, at least one government has admitted that it has been withholding data that may link the COVID jab to excess deaths. Of course, this news is nowhere near new. We knew they were hiding data at least three years ago:
Those who released information that COVID itself was manmade or that the vaccine was ineffective were summarily deplatformed, fired, and otherwise had their lives destroyed. There is nothing so evil that our government won’t do it.