Once my employer stopped paying nurses bonus money for coming in when staffing was short, nurses naturally stopped coming in. I know I did. I stopped taking extra shifts, because my time off was worth more than the little bit of extra cash. I mean, I only work one day per week, sometimes two if I feel like it.
So now the ED is back to a staffing shortage.
So badly that I was called this morning and asked to work an extra shift today. I turned it down, because I am already working four 12 hour shifts this week, and had been cheated out of two of my three bonuses I was told I could have until they cancelled the bonus system.
So then they offered me a $25 per hour bonus if I would come in. OK, so I am working 60 hours this week. That’s just more money in the IRA for the future. I can be a whore like that sometimes. I guess they need to keep the emergency room open more than they need to save money.
A couple of examples of people being shady and not doing honest business on a handshake. The first is:
Because I am no longer a full time employee, there are benefits I no longer receive. One of them is insurance, so I just bought life insurance on my own. We don’t have a lot of debt, so two months ago, I got a small policy: $100,000 of insurance. I applied and got several offers from different companies. One of them came up with a quote for $1300 per year and received a letter that I would be covered for $25,000 until my physical exam, after which it would be increased to $100,000 unless issues were discovered. I paid the first year in advance, lump sum. This morning I found a letter in my mailbox, dated two months ago on the face of the letter, but postmarked three days ago. It said that due to my diabetes, they can insure me, but at a higher rate, and they would bill me for the increased rate. I disclosed the diabetes in my application, and I still haven’t had the physical exam.
Maybe the fine print gives the company the legal right to do this. That isn’t my point. My point is that the company knew about my diabetes when it quoted the price, accepted my payment, and told me the rate could change if the physical uncovered a problem. No physical ever took place, and no new problem was discovered. Changing the price under those circumstances feels less like underwriting and more like bait-and-switch. The problem is insurance policies are long, complex legal documents backed by a large insurance company with tons of lawyers on staff. You take what they give you, and don’t fight. Any fight will be long, expensive, and will involve some sort of legal exemption buried in the 40 page legalese of the policy. They are free to screw you as they see fit.
The second involves my employer. First, an explanation of how nursing scheduling works. This is how it works at every hospital I have ever worked at: The schedule comes out for 6 weeks at a time. When the new schedule opens for bidding, nurses can begin bidding for days on the schedule, full time first, then part time, then PRN. You can place bids for available to work, want off, PTO.
That is, for two weeks, full time employees get to ask for schedule changes. Let’s say you are a full time and normally work Monday, Tuesday, Thursday, but your kid has a dentist appointment on Thursday, so you request M-T-W this week. You would put in a bid for available to work Wednesday, request off for Thursday. As long as there is a spot, you get it. Alternatively, you could request PTO for that day, but that’s burning vacation for nothing.
Then for a week, the part time nurses bid for days that are left. Finally, the PRN nurses do the same for a week. After the four weeks of bidding are done, the schedule closes. The scheduler spends a week balancing and filling slots, then the schedule is posted. Once the schedule closes, no more requests are allowed. If you are assigned to work a day and can’t work, you either have to call in sick or find someone to swap shifts, which almost never happens.
Alright, so that’s the background.
You also know that recently, we haven’t had enough staff. It’s a regional problem- three different ED’s in the area that are part of the same hospital chain are critically short of nurses. They started offering bonuses for working extra shifts. I piled them on, and wound up working eleven bonus shifts in a single schedule. I collected nearly $5,000 in bonus money for picking up extra shifts.
When bidding began on the new schedule, I signed up for a total of eighteen extra shifts in a six week schedule- that’s 24 days of work in six weeks. One week, I am working five 12 hour shifts. Hey, I figured the bonuses wouldn’t last forever, and my wife is back to school as a teacher by then, might as well make some extra money. That would wind up being more than $23,000 in a six week period.
The day after the schedule was closed, my employer made an announcement: No more bonuses until you’ve worked 36 hours in a week. In other words, any full time employees get bonuses for every extra shifts, but part time and PRN dont get any unless picking up multiple extra shifts.
Whatever, I knew bonuses wouldn’t last forever. The prolem is the schedule is closed, so you still have to work the days you signed up for, but aren’t eligible for the bonuses that made you take them in the first place. Here is the closing of the email we got:
If you are interested in increasing your hours or exploring full-time opportunities, please reach out to management to discuss available options. Thank you for your continued dedication to our patients, your teammates, and our community. We are grateful for your commitment and the important role you play in delivering exceptional care every day.
I don’t care that the bonuses went away. We all knew they would eventually. What makes it shady was removing the bonuses AFTER people had volunteered to pick up the slack and telling them they can’t cancel the extra shifts. I value time off enough that I’m not interested in full time. I’m mercenary like that.
It’s enough of a “screw you” to anger everyone, but not enough of one to make you quit. What it does mean is that I won’t take one hour of extra shift unless I already have the details in writing, lest the deal get changed.
The part time and PRN nurses are all of the opinion that management deliberately waited until the schedule’s bidding process was closed. That locks the nurses into extra shifts for the last two weeks of the current schedule and the entirety of the next six week schedule, but without the employer having to pay the promised (and now retracted) bonus money. Eight weeks of nurses picking up extra shifts for a fraction of what it would cost to pay the promised bonuses.
Dishonest. Unethical.
OK, you got me. I am not going to quit over this, it’s not that big of a deal, as I still get my regular and overtime pay for it. However, it also means that I am highly unlikely to do you any favors in the future.
And don’t call us a team, because teamwork is a two-way street. Your employer isn’t your friend, they aren’t your buddy. This is a business arrangement, and I don’t come here because we are friends. I’m here for the money.
Both organizations made representations designed to influence my decision. After I relied on those representations, in one case by paying the premium, and committing to extra shifts in the other, they changed the terms while treating my commitment as irrevocable. Maybe their paperwork allows it. Our legal system means the fight is harder than the reward justifies. That does not make it honest. Nor does it make you ethical.
This is just how business is done nowadays. Get money however you can, and screw the other guy if he doesn’t like it. That’s his fault for being a gullible rube and trusting you at your word.
Years ago, when I was still a paramedic with the fire department, we would occasionally draw blood from patients and turn it over to the police. More than once, I drew a resisting patient’s blood while a police officer held a taser to their neck.
Why would I do that, you ask?
Florida has long had a specific statute, § 316.1933, covering crashes involving death or serious bodily injury. It provides that when an officer has probable cause to believe an impaired driver caused a death or serious bodily injury, the officer shall require a blood test. The statute also expressly authorizes the officer to use reasonable force if necessary, and it authorizes physicians, nurses, paramedics, and other qualified personnel to draw the blood at the officer’s request. It also grants immunity to those assisting with the draw when acting under the statute at the direction of a law enforcement officer.
For many years, the prevailing view, based largely on the earlier U.S. Supreme Court decision in Schmerber v. California (1966), was that alcohol dissipating from the bloodstream created an exigency justifying a warrantless blood draw in many DUI cases. The person’s liver was literally destroying the evidence every minute, and the delay in obtaining a warrant was the difference between a DUI homicide and a drunk walking away.
I understood why the law was there, and I also disagreed with it. My favorite quote is “better 1,000 guilty go free than 1 innocent person be convicted.” The truth is that the DUI law changes have had no discernible effect on the rate of traffic fatalities. Of course, the fact that the government uses traffic offenses as a cash cow, with Florida making $100 million a year from traffic tickets has nothing to do with it. In California, it was discovered that 1,600 DUI checkpoints yielded only 3,200 DUI arrests (two per checkpoint), but resulted in $40 million in traffic tickets and 24,000 vehicle confiscations. Cops also won, being paid $30 million in overtime to staff the checkpoints.
That was the law when I retired from the fire department in 2011. Then in 2013, the Supreme Court decided Missouri v. McNeely. The Court held that the natural metabolization of alcohol by itself does not automatically create an exigency. Instead, officers generally need a warrant unless the facts of the particular case make obtaining one impractical.
This is a holiday weekend, where I make time and a half plus bonus money. All of it together has me making more than $100 per hour. So I am busy, and when you work multiple shifts, there isn’t time for much else.
0700 Wake up, cook eat and clean up from breakfast, shower, get dressed
0900 Out the door
1000-2200 work
2300 home
2330 in bed
Do it all over again. Note that there is no time for blogging. Will resume on Monday.
In the ED where I work, I am one of only 18 nurses who work there. Two of those 18 nurses are PRN (I am one of them). Of those 18, two of them just got transferred to a different location, one just took a job in another department, and two quit. Doing the math, we just lost a quarter of our nursing staff. That tends to happen with nursing- it’s difficult to find good nurses, and competitors try to hire them away.
They are trying to hire more and have had a few interviews, but no one who has been offered the job has accepted. I’m guessing it’s because nursing pay in the area has climbed again and my employer is offering less than the candidates are being offered elsewhere. They will be forced to raise starting pay again, which is the only way to get a raise- about every two years, change jobs for more money.
At any rate, we still need to staff the place, and to do that, management has declared a critical need. When they do that, the bonuses come out. For the months of July and August, any shift you pick up in addition to your contract gets you a bonus: $33.33 per hour ($400 for a shift) on weekdays, $41.67 per hour ($500 for a shift) on weekends. Since I am PRN, I am only contracted to work one day per week, meaning that I get that bonus for every day that I work in a week beyond that first one. Even if I only work full time hours, I get $800-$1000 per week in bonuses.
The best part is that it is the slow season for emergency departments around the state, so our workload is low. High pay and low work? Of course I jumped on it. I am working a bunch this July, but I am going to make about $20,000 this month alone. When the August schedule gets done, I will try to do the same.
That just adds to the retirement fund. I will be busy, but still working less and making more than I would if I were full time.
One of the things you learn when driving fire trucks is called “protecting the scene.” As the driver of a large piece of fire apparatus, you park it at an angle across the lane of the road where your crew is working and the one adjacent to it. You angle the front tires in such a way that, should the rig get struck, it won’t be pushed into your crew. A Fort Worth fire crew recently demonstrated why this idea is so important. The driver of this fire truck likely saved multiple lives when he did this.
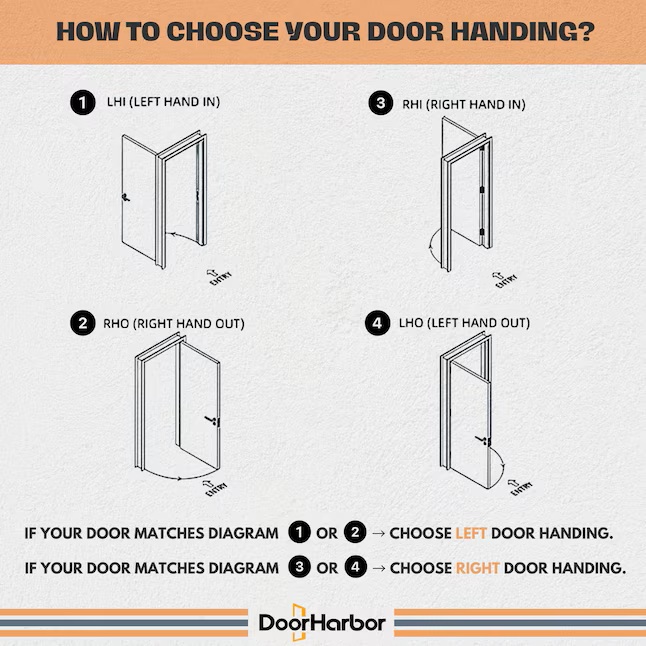
My wife decided that the pantry gets too warm. There isn’t a register in there for air conditioning. We looked at several options, and the one that was easiest and cheapest was to replace the pantry door from a two panel door to a louvered door. Lowes had the doors on sale for $415, so I figured that was the cheapest and best way to go. When I ordered the door, I was asked how I wanted the door cut for hinges. Here is the diagram:
Standing outside of the pantry, the door opens towards you with the hinges on the left and the door handle on your right, just like (4) LHO (Left Hand Out) in the diagram above. It says order right door handing, so that’s what I ordered.
Two days later, I got a text from the manufacturer with a copy of the diagram above, asking me how I wanted the door cut. I responded with “Left Hand Out.” They replied: “Well received. Thank you for the confirmation.”
Two weeks I waited for that door. As soon as it got delivered, I started to put the hinges on the door.
They are cut on the wrong side. The hinges are made for a left hand door. Now Lowes handled it well, telling me that I could return the door to the closest store, or they could schedule a pickup. I am bringing the door back to the store.
Now I have to reorder the door. That’s going to mess up my schedule, because I have a lot going on. I may have to wait to reorder it because I won’t have time to deal with it on July 4th weekend.
There are other things happening that are causing a lot of upheaval in my house right now. I will expand upon them at a later date, but let’s just say that I have a lot of issues on the agenda right now, and I feel like my schedule is filled to capacity.
My Father in law needed some help throwing sod in his yard today, so I wound up spending the day helping him with yard work. I have told the in-laws not to do that sort of work, but to call me instead. They fall quite often, and I don’t want them getting hurt.
I spent about 8 hours throwing sod and working in their yard. It was 95 degF today, so I am spent.
Family comes first. Let’s see what we can do tomorrow.
I have had some really shitty bosses. My last two employers, while creating shitty working conditions and a bit of wage theft, weren’t even the worst of them. I had a boss once at an ambulance company who wouldn’t let us have food and water in the ambulance, and wouldn’t allow us to have meal breaks. His saying was “I don’t pay you to eat lunch, I pay you to transport patients.” His other (in)famous quote was, “The customer is always right. In our case, the customer is the nursing home, doctor’s office, or hospital that hires our service. It’s not the patients, the patients are cargo, and no one cares what cargo thinks.” He eventually got caught committing Medicare fraud and was forced to reimburse the government some of the money (about 25%) that the Feds accused him of stealing. Yeah, real nice guy.
It was that guy, more than most, who convinced me just how corrupt the government is, especially at the Federal level. It’s also about as rare as hair on a frog’s ass to see anyone get anything over on these kinds of people. It seems that crime DOES pay, if you are friends or coconspirators with the guys who decides what a crime is.
There was one boss that I really wound up getting a bit of payback, and it’s a great story. This was back in the late 90s, while my divorce was pending. I worked for a steel mill back then, and the steel mill went into bankruptcy. They made the announcement at quitting time. They told everyone to shut down the machines, stand in line, and clock out for the day. As you clocked out, they handed you your last check and told you whether or not you would still have a job. As the maintenance manager, I didn’t get laid off that round, but some of my employees did. Many of them complained that their checks were shorted.
One of the employees who got laid off was the girl in charge of the tool crib. It was her job to watch over the tools that employees could sign out, and ensure that the employee signing them out actually brought them back. There was some expensive stuff in there: welders, plasma cutters, some tool sets were thousands of dollars in value. Once she was gone, the employees who were left figured that those tools were free for the taking, and taking is exactly what happened.
A month later, it was my turn to be laid off. When they let me go, I was told that one of my employees would be taking over my job. He had been trying to get my job since I started there- even going so far as to sabotage things and then fix them quickly, pointing out that I wasn’t as good or as fast as he was. It’s easy to find the problem when you are the one who broke it. He would do things like move a wire in a control device from one terminal to another after taking all of the wire labels off. That was a tough thing to find. Trust me, this is important later.
Anyhow, they laid me off and claimed that since I was responsible for all of the tools that were now missing, I could consider that to be my last paycheck. I got screwed out of 2 grand or so.
A few months passed. In the meantime, I was homeless and really hurting for money. At this time, I was living in my car. I had a second job, picking up garbage after the Shamu show at Sea World. That paid less than $7 an hour. I bought a car at a “buy here, pay here.” I wasn’t eating much, I couldn’t afford it. I showered at work. As a perk of the job, the city allowed us to use the gym at the civic center for $20 per month. I joined so I could take showers at the gym. I worked out a lot because the gym was air conditioned.
One day, I got a call from the vice president. It went like this: “Dive, this is Stan.” Me: “What do you want?” Stan: “I have a problem, my number two line is down and Sonny can’t find the problem. I’m losing $2,000 an hour.” Me: “Yeah, you have a problem all right. It sucks to be you.”
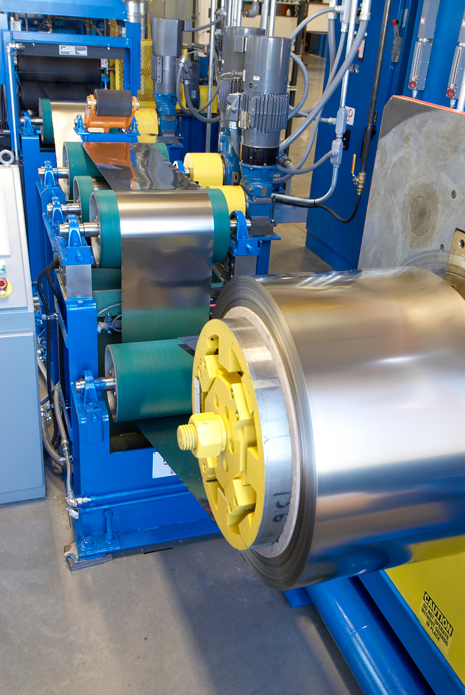
Line two was a large pipe machine. It would take rolls of flat stainless steel and roll it into a tube. The ends of the steel would be welded together with a strong (50kw) microwave welder, then it would pass through a high frequency annealer that would heat the pipe using radio waves to temper the pipe. These things are fast- the high speed line was capable of making over 100 feet per minute of 1 inch stainless steel tubing. It’s all controlled by a microprocessor, and some of the electronics can be complicated. The pipe is pulled through the mill by a pair of 100 horsepower electric motors mounted on large transmissions.
So it turns out that I am pretty much the only guy in the entire state who knows how to repair stainless steel cold rolling machines with microwave welders. He is desperate. He practically begged me to come and help him. So, I told him that I would come and fix the machine for the 2 grand he owed me, any parts that were needed, plus a thousand bucks in a flat service fee, and I wanted the money in my hand before I would touch anything. He immediately replied, “Fine, as long as you are here within 90 minutes.” Damn, he didn’t hesitate, I must not have asked for enough.
So I was there in just over an hour, and it was an easy fix. He handed me $3000, I replaced a blown fuse, reset the microprocessor, and the machine started right up. Sonny was livid: “Demand your money back, he didn’t do shit. All he did was change a fuse and push two buttons! I could have done that!”
I looked at Sonny and replied: “So if you could do it, why didn’t you?” His answer was that he didn’t know which fuse to change. I laughed and said, “That’s what costs money- knowing which fuse to change and what buttons to push.”
That $3k really helped. It was two months’ pay at my other two jobs combined, and it was under the table money that the ex-wife couldn’t get her greedy fingers on.
Over the next year, I would get called over there to fix things from time to time. The charge was the same- $1000 per visit, flat charge, for up to two hours of work, then it was $250 per hour after that. I was working 3 or 4 days a month and making as much as I had been while I was working there full time. This gig helped me to be able to eat and eventually get an apartment with a roommate. I will admit that I did feel guilty at one point, and offered Stan a service contract where I would come out one day per week for $500 per week, plus emergency calls at $500 per visit. He said no.
One of the calls was because his eddy tester was broken. The plant had this eddy tester that you would run a pipe through, and it would test the integrity of the weld. The tester was connected to a PC with a proprietary expansion card. You can’t ship ISO certified welded pipe without it. Theirs was broken, and the company that made it charged portal to portal for service visits. It was expensive to have the factory guy come out, and he wouldn’t arrive for a couple of days.
I got there, and it turns out the motherboard of the PC was fried, but the expansion card and sensor was working. So I went to Stan and told him I would fix it that night, but it was going to cost him $5000. He paid it, and I fixed it by running home and grabbing my own PC to use as parts. The next day, I went and bought a new PC for only $1000. Some of my coworkers at the fire department told me I ripped him off by selling him a 2 year old PC for five times what it was worth. Whatever, he had a choice, and it still cost him less than it would have cost to have a factory guy come out, so I had no problems sleeping in the apartment I shared with my roommate.
The place finally shut down, but I got my money’s worth. The funniest part of the story was the two guys who owned the company went on to open another business a year later, and hired me to do some side work in their new place. I cut them a deal- I did the jobs for slightly less. One of those was putting a rotary phase converter into the place so he could run three phase motors on single phase power.
The extra cash I got from those guys was a big help when I needed it, and it was a bit of payback for how they screwed me on the way out.
This story is part of the reason why I get angry when the GenZ faggots tell me that I had it easy, and how hard their lives are now. Those blue haired commie idiots wouldn’t know hard knocks if it pushed a broomstick up their ass.
I now work for a free standing Emergency Room. The regional manager had mentioned during my interview that they were opening a new location this summer, and asked if I would consider taking over as the manager, or was I wedded to just being PRN. I told her that would depend on the terms of the offer. I’m guessing the current managers consider me to be a threat, at least judging by what has happened since.
I had worked a total of 7 days at my new job since completing onboarding: one or two days per week, not counting the three weeks of the Europe trip. I got called into the office by the site manager. On her computer screen, the ED manager from the other site where I did my onboarding was there via TEAMS. The manager looks at me and says “How do you think you are doing?”
I said, “Well, I would have said fine, but since we are having this meeting, I’m guessing that’s not right.”
Both laugh. Then the manager continues, telling me that she has had “people” come to her and tell her that I am taking too long to triage my patients. I tell her that this is concerning to me, and I am more than willing to increase my speed, if they can tell me where I am lagging. No one wants to be “that guy” who no one wants to work with.
They tell me they have no idea. The manager attending by TEAMS says, if only there was some way we could get data from EPIC (our medical charting software) we would be able to tell you. I wish EPIC had a report for that.
“It does- there are reports for everything a nurse does- triage time, treatment efficiency, average time to complete medication orders, all of it. Let me show you how,” I offered.
The manager replied: “Well, we aren’t sure that those reports are accurate. There are ways to game that data.”
So then I asked them where I am slow, and what I can do to show improvement. They tell me that they don’t know. Then they instruct me to go see nurses Amy and John, who are working with me that day. They can watch me work and tell me. They tell me that the standard is for the patient to wait 2 minutes or less in the waiting room, and 10 minutes or less for triage. The expectation is that I comply with those numbers. Then they thanked me for not being difficult and accepting the counseling like a professional.
So I took their advice and went to see Amy and John. That’s helpful, because Amy has worked with me for 4 of the 7 shifts I’ve had so far. They were both surprised, and told me I wasn’t slow, and couldn’t see anything I was doing wrong.
So I turned to EPIC- you know, the ones the manager at first said didn’t exist, and then told me weren’t accurate. According to EPIC, there are 18 nurses in my department. I ran a nurse efficiency report. The report showed the nurses have average triage times ranging from 2 minutes to 9 minutes, with an average of all of them being 4 minutes and 32 seconds. My average time? 4 minutes and 3 seconds. Not one of my patients has been longer than 8 minutes. In addition, I see more patients than my coworkers on the days that I am working, which indicates that I am faster than they are. Not more than any one of my coworkers- more than they are combined. On the days I work, I see 55% of all patients who walk through the door. The other two nurses on shift with me see the remaining 45% combined. I’m fast enough that coworkers tell me to sit down and let them catch a couple of patients.
So I sent an email to the manager informing her that Amy and John had no suggestions, and EPIC showed my average times to be far below the required ten minutes. I then asked if they could be more specific, because I cannot correct a deficient behavior if my leadership can’t even tell me what behavior it is that I need to correct. I attached a copy of the report.
This is some piss-poor management. They complain that my work isn’t sufficient. They can’t tell me what exactly I’m doing that is deficient, nor can they tell me how to correct that deficiency. Instead they send me to talk to a pair of coworkers for advice, who also can’t see where I am doing anything wrong.
What management school is that?
In this case, the email I sent was for documentation purposes. I only work there one or two days a week. They had talked to me about joining the management team, but I don’t want to go full time again, no matter what the pay. I’m going to keep my head down and do three to five more years working part time, then collect social security. I am no longer fighting the workplace wars that are so stressful and aren’t that important.
It’s been over a month since all of that took place. No one has said a word, and I received no answer to my email. I suspect that my MBA, the fact that I am more certified than my managers, I am more knowledgeable on the EPIC software as evidenced by her not even knowing how to run the nurse efficiency report, and let’s face it, because I am a man, all make me a target.
I’ve been watching my coworkers. One of the ones who has a 2 minute triage average? Yeah, when a patient walks in, he moves them in the computer from lobby to a room, then charts his entire assessment and triage. All without getting up from his desk. Then he goes to the lobby to actually put the patient in a room, enters vital signs, and collects any needed labs. In other words, he isn’t fast, he is lying. He isn’t doing his job, he is just reporting that he is doing his job. That is something I refuse to do. This is what happens when management cares more about metrics than outcomes. Too many administrators are like that, but I just won’t do it. Reports are supposed to reflect reality, but too many nurses bend reality to fit what the reports show.
So my plan here is now: No write-ups, no escalations, no drama, not being the fastest, best, or most efficient nurse. Keep my head down, collect my $50 an hour, and go home at the end of the day. If someone says something to correct or counsel me, the answer will be “Got it—I’ll keep that in mind. Thank you for your input.”
Things are winding down as I glide into retirement. In January, I sold the rental properties and paid off my house. I need to earn enough this year to cover my capital gains from that on next year’s taxes. Next year, I pay off my Jeep Gladiator. Then I keep putting money away to fund my future travels. I don’t need to be right, or be the best, I just need to be paid. Keep my eye on the prize. Let them all keep fighting over who is the best and playing office political games. I’m not playing those any longer.
I only have three years before I can retire. After that, I only work until I get tired of the bullshit.