The Republican party shows its true colors: No sell out is too large or too egregious, if it means that I can get enough lefties to vote for me. Selling out, the tactic of the Republican party. Too bad the rules are rigged to prevent another party from becoming viable.
Uncategorized
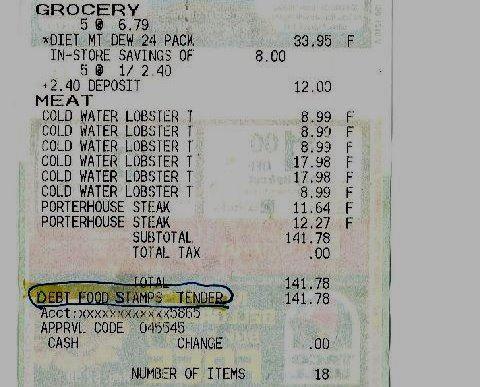
Found in a parking lot
Here is a food receipt recently found in a parking lot by a friend, and emailed to me:
5 cases of diet Mountain Dew, 8 lobster tails, 2 Porterhouse Steaks, total grocery bill of $142. All paid with an EBT card.
About 100 million people in the United States are receiving some sort of government money. At the beginning of this year, only four of the 80-plus federal welfare
programs had work requirements; the Obama Administration has now
suspended the work requirements in two of these. After the Obama
Administration suspended the work requirement from the food stamp
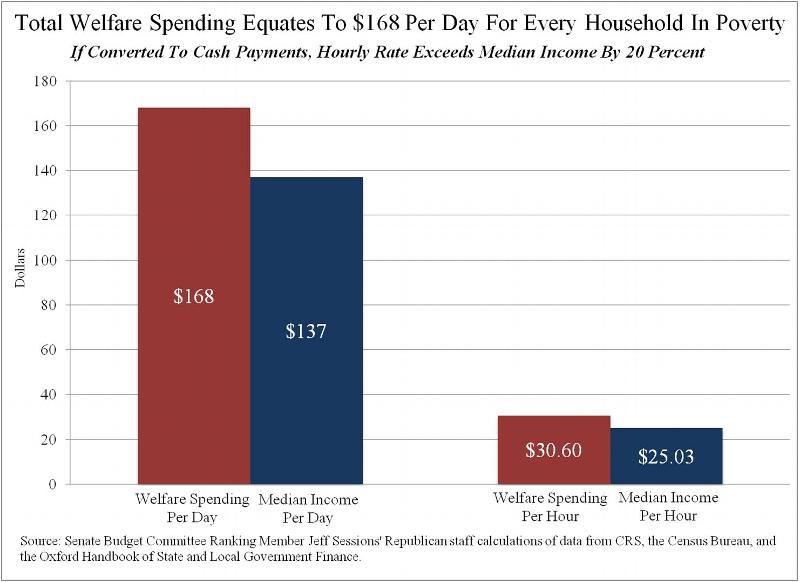
program in 2009, the number of people on food stamps doubled. In fact, if you take the trillion dollars spent on welfare programs and divide it by the number of people receiving them (100 million), it comes to $100,000 spent for each person receiving aid.
Welfare pays more than an $8 an hour job in 40 out of the 50 states, and this figure doesn’t include food stamps and Medicaid. The government spends an average of $168 for each person on welfare.
Welfare now surpasses the government’s biggest traditional money pit, the Pentagon. “By 2022, there will be $2.33 in federal and state welfare spending for every $1 spent on national defense.” Our National debt, as listed by the treasury, is $6.5 trillion higher than it was when Obama took office.Our debt has been doubling about every 8-10 years for every president except Clinton. Clinton added 140% to the debt.
It gets even worse: Much of the spending and borrowing is being paid for by monetizing the debt. The Federal Reserve is busy buying US treasuries. This is called monetizing the debt.This will eventually begin to hurt the value of the dollar. The only reason that this hasn’t already begun is that so many commodities (like oil) are pegged to the dollar, because the dollar is the reserve currency. One that changes (and it will) the days of runaway inflation will arrive.
Uncategorized
It takes a village
In June 2012, a man named Joshua Hakken was arrested for possession of marijuana. Joshua and SharynHakken, who media outlets continue to describe as
“anti-government” due to their anarchist/libertarian postings on
firearm and homeschooling forums, had their parental rights terminated by a judge. At the time, according to investigators, the couple lost custody of the twoboys after attending an anti-government rally in Louisiana.Investigators now deny that charge.
One of the things he allegedly wrote was this:
“My name is Joshua Hakken,” he wrote. “I am a father, a
registered professional mechanical engineer and a veteran of the
USAF. I am absolutely devoted to life, liberty, the rights of the
individual and the Constitution of the United States of America.
“
After saying that he had noticed that “things here in Florida
have not added up for quite some time,” he concluded, “in these
crazy times, maintaining open communication lines for ideas,
observations and news is absolutely crucial if the ‘good guys’ are
to be successful in surviving to maintain the fight of ideas.”
Not worse than what even mainstream people like Rush Limbaugh or Glenn Beck are saying.
The police also claim that Joshua also showed up at a Louisiana state run foster facility with a gun and tried to gain access, and when unsuccessful, left. I find this hard to believe. If this were indeed the case, why wasn’t an arrest warrant issued then?
So Joshua and Sharyn began to activate a daring plan to recover their children. They bought a 25 foot sailboat and were
seen loading supplies onto the boat in the John’s Pass marina, located
in the Tampa area.
In the early morning hours of April 3, Joshua and Sharyn entered the home of Sharyn’s mother armed with at least one handgun, tied up Sharyn’s mother, and took the kids.
. The Hakken children were listed as the “victims” and their parents were listed as the “suspects” in an abduction. On April 4, acting on a tip, Hillsboro County Deputies found the Hakkens’ SUV in a parking garage near the John’s Pass Marina.On April 5, a witness came forward and said he spotted the boat passing under a bridge near the John’s Pass Marina, and heading out to sea. The search expanded. Police tried to locate their cell phones, but they had been turned off. Police then expanded the search to the sea, and to four states.
Rumors circulated that the family had fled to Cuba. It was then confirmed on April 9 that the Hakkens were in fact, in Havana, Cuba. At least one Florida attorney believes that the children will not be extradited. I say good for them. Taking someone’s kids for a marijuana arrest? MY hat is off to him for protecting his kids.
This is what it means when authorities say that your children are the property of the state. It takes a village…
Uncategorized
Swiss Guard
When I posted about the Swiss Guard the other day, it caused me to get into a discussion with a Catholic friend, who accused me of posting a fake photo and lying about the Church. This caused me to embark on a research campaign throughout the Internet, looking for evidence of the modern arms carried by the Swiss Guard. That was not easy. The Catholic Church is largely run by people who know how to keep a secret. Ever meet a Jesuit that couldn’t keep a secret?
Anyhow, during my research, I found quite a few places where people made fun of the guards because of their quaint ceremonial uniforms, and people saying that they must be incompetent. I would point out that those uniforms are CEREMONIAL, were designed by Michelangelo himself, and are meant to be seen as non threatening. Pope Paul the 6th is said to have begun a campaign of making the Guard appear less threatening, to the point where it was suggested in 1968 that the halberds, chest plates, and helmets would be eliminated. That doesn’t mean that the Guard doesn’t know its business. They have guarded the Holy See for over 500 years, and not one Pope has been killed under their watch. That is an impressive record that no other security detail in the world can come close to matching, although they came close to losing that unblemished record when Pope john Paul II was shot in 1981.
In order to be a member of the Swiss Guard, the applicant must be a Swiss citizen of Roman Catholic faith, be between 19 and 30 years old, have attended the Swiss military academy, unmarried, and at least 174 cm tall. New guards are sworn in once a year, on May 6th.
They carry modern weapons, and by all accounts appear to be a well trained, well equipped force. I may have a problem with the Church’s policies, but the training and record of the Swiss Guard is exemplary.
Uncategorized
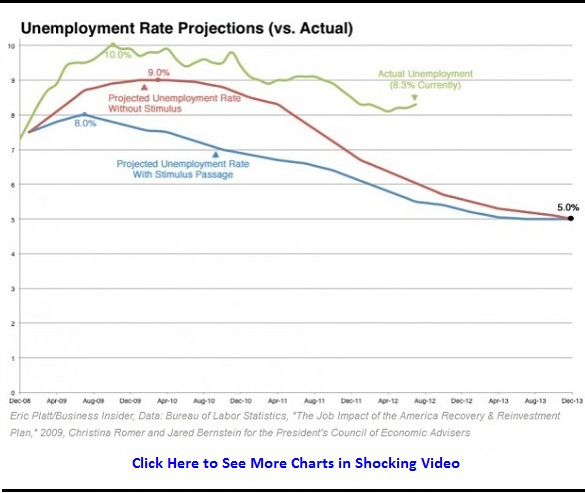
Forward!!
Next time someone blathers to me about how Obama has turned the economy around, and that we have recovered:
Uncategorized
Restricted rights
There is an old story from back in the days when states required people to take a test in order to vote. Back in those days, it was the sheriff of the county that administered the test in the state of Georgia. the test was simple: The sheriff would hand the applicant a newspaper, and simply read the headline aloud.
Now the story goes that one day, a black man appeared at the Sheriff’s office and wanted to register to vote. The sheriff handed the man a newspaper.
It was printed in Japanese. Without missing a beat, the man said: “Well, this is easy. It says here that there ain’t no niggas gonna be allowed to vote in Georgia this year.”
This is the reason that we do not restrict rights in this country: because to restrict a right is to allow people to deny that right to others. This is why THIS post rightly pisses me off. The racism that allowed that sheriff to deny the man his voting right is just as repugnant as the attitude being used to deny gay marriage or deny gun rights. How dare you restrict a right in order to force others to live as you wish them to.

Uncategorized
Church hypocrisy
So the Catholic Bishops of the USA have recently come down on a position whereby they have declared that it is a sin to own weapons, and call on all Catholics to support gun control. Here is a copy of the actual declaration, as sent to the US Senate.(PDF Warning)
The money quote:
The Vatican’s Pontifical Council for Justice and Peace, in their document, “The International Arms Trade (2006),”emphasized the importance of enacting concrete controls on the production, possession, and trade in weapons, including handguns,calling for them to be regulated” by paying due attention to specific principles of the moral and legal order.”
This comes from the Church that owns a room full of swords, machine guns, and other firearms for the Vatican’s Swiss Guard:
Also, this would seem to preclude the owning and carrying of swords by the Knights of Columbus:

One reader of this post on the subject pointed this out in comments, and the reply was:
I think it would depend on how many people have been killed by those K of C ceremonial swords when deciding whether to ban them.
More people have been killed by swords than by privately owned firearms, and no one has been killed by any gun that I own. By that standard, my guns shouldn’t be illegal.
Uncategorized
Common use test
In the majority opinion of the Heller case, the Supreme court said:
“We also recognize another important limitation on the right to keep and carry arms.
Miller
(an earlier case) said, as we have explained, that the sorts of weapons
protected were those “in common use at the time”. We think that
limitation is fairly supported by the historical tradition of
prohibiting the carrying of ‘dangerous and unusual weapons.’ ”
This has been called the “common use” test. This can be a dangerous precedent, because what is not in common use today may be the best thing tomorrow. Case in point:
A doctor in London thinks that he can use psilocybin, the psychedelic ingredient in magic mushrooms, to treat depression. However, the problem is that the drug is a class I controlled substance, meaning that it is highly addictive and has no recognized medical use. For that reason, scientists and doctors cannot even use the drug in studies to investigate whether or not it has a medical use. In other words, since it is not in common use, no one may use it, even to find out if it CAN be useful. That is the problem with “common use” tests.
This line of reasoning means that the founding fathers meant for the Constitution to only protect muskets, as they were all that was in common use at the time of ratification. I cannot believe that the founders could possibly be so short sighted. If this were the case, the First Amendment would not protect your right to speech on the internet, over the telephone, or on the radio.
Here in the US, the Republican party is all for drug prohibition and fully supports this application of the common use test. Marijuana is itself a class 1 controlled substance, and the Republicans refuse to admit that it has, or ever can have, a legitimate medical use. The Republicans: for smaller, less intrusive government. Unless it involves drugs. Or sex. Or marriage. Or forcing people to learn about religion in school. Or making alcohol off limits during the hours that church is in session. Or…
Uncategorized
Idiots
This anti-gun screed is so full of fail, it is sickening. Drop by and give him your opinion.
Uncategorized
Real inflation
I read an article yesterday that claims the rate of inflation in the US is 1.3 percent, and 10 year treasury yields are holding at 1.69 percent. The two are tied together, and they are both being manipulated.
The official inflation numbers are being massaged. They exclude energy and food, which is a major part of our expenses. Let’s take a look at what energy and food are doing. This website began tracking the prices of 30 grocery items, plus a gallon of gasoline in 2008. What they found was the cost of these items was:
$54.11 in 2008.
$70.37 in March of 2011, an inflation rate of about 9%.
$76.86 in August of 2011, meaning an annual inflation rate of about 18%.
$79.28, in September of 2012, a 3% inflation rate.
The only thing that has slowed down inflation is the cost of housing from 2008-2009, with the crash of the housing market. That has since corrected itself. Look at the prices here.
Interestingly, average wages in the US are 20 times higher than they were in 1930.
A new house is 62 times more expensive
A new car is 47 times more expensive.
Gasoline is 21 times as much.
Bread 31 times.
Beef 33 times as much as 1930.
In terms of real purchasing power, this is the poorest generation in over 100 years.