This is a story of a patient from a year or so ago, while I still worked for my last employer.
A patient comes in because he has had increasing shortness of breath for about two weeks. He was walking down a small hill from where he parked his motorcycle and fell, tumbling down the small incline. He fell about 10 feet or so, he says. His vitals look fine. He is a bit of an overweight guy, typical 60-something man trying to recapture his youth by riding a Harley.
So I ordered a chest x-ray, started an IV, and did his intake paperwork. No doctor is signed on to his case yet. If the x-ray shows anything significant, the technician who takes it will normally give me a heads up. He didn’t in this case. The image of the x-ray came up on my computer, I took one look at it and immediately flagged down the first passing doctor and said, “Hey, I know that you’re busy and this isn’t your patient, but you need to see this now.” Here is what it looked like:
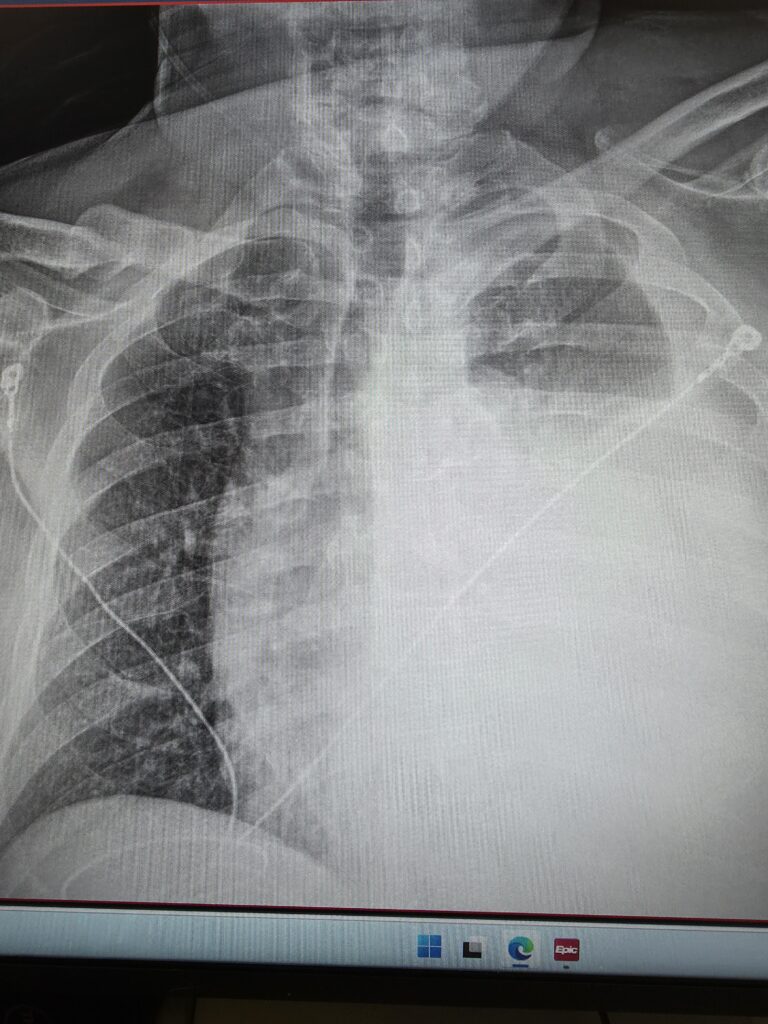
In case you don’t know what you are looking at, the dark section on the left is a relatively normal looking lung. The heart and trachea are supposed to be on the right side of the image and are being pushed into the other side by the large amount of blood that is collapsing his left lung (which appears on the right in this image). If you look closely at the film, you can see all of the structures that are supposed to be midline are being pushed over. This is called a hemothorax, and is a life-threatening medical emergency where a massive volume of blood rapidly accumulates in the pleural space (the area between the chest wall and the lung). This buildup compresses the lung and puts dangerous pressure on the main vein bringing blood to the heart (the vena cava) and the heart, leading to cardiovascular collapse, severe respiratory distress, and shock.
The doctor took one look at this and said “Holy shit! I’m signing up for him. Get me set up for a chest tube and some conscious sedation. Call respiratory and let’s get ready to send him to a trauma center.”
The patient had a rather chubby neck with a beard so it wasn’t readily apparent, but if you put the finger of one hand on his Adam’s apple, and a finger from the other hand in his sternal notch, you could see that his windpipe was deviating to the patient’s right. He was a good sport and didn’t even mind that I brought a couple of new nurses into the room to see what a tension hemothorax looked like. Of course, he had no lung sounds on the left, and his heart tones were distinctly muffled. His pulse pressure was a bit narrow.
There were not any other nurses or respiratory technicians available to help in time, so I grabbed a nursing assistant and the three of us (doctor, myself, and aide) rapidly initiated conscious sedation and inserted a chest tube. That’s a handful for one nurse and a doctor to handle (the nurses aid is pretty much there to hold this, and hand me that and isn’t much of a help)- I had to administer sedation, monitor and maintain his airway and breathing, and chart everything. For one nurse to do all of that without help is a major safety issue, and is one of the (many) reasons why I don’t work for that hospital any longer. That place is just understaffed to the point of compromising patient safety.
Once we got the tube in place, we sent him for a CT scan, and it turns out he had 4 ribs broken in two places- a classic flail chest. If you put your hands on his rib cage, you could feel the paradoxical motion of the chest wall. This is incredible, considering that he walked in to the ED and had been walking around like this for two weeks. The video below shows you what paradoxical motion looks like, but my patient’s wasn’t quite as pronounced as the video (and was located under his left armpit).
Anyhow, I pulled about 2 liters of blood from his chest cavity before we crimped off the tube because we didn’t want him losing too much blood. A helicopter came and took him to a trauma center, and the trauma surgeon was still pissed because we took out so much blood.
The patient made a full recovery.
5 Comments
ghostsniper · June 10, 2026 at 6:13 am
Jeez, that’s some pretty “violent” breathing in that vid. I never seen ribs bend that way. Like they separated from the sternum.
Divemedic · June 10, 2026 at 6:21 am
That’s exactly what happens in a flail chest- adjacent ribs are broken in two places- this allows that section of the chest wall to “float” without connection to the sternum or the spine. As pressure changes inside of the chest during respiration, the flail segment moves opposite the direction of the remainder of the chest wall.
SP RN · June 10, 2026 at 10:35 am
1. ‘Conscious sedation’ is mis-named: if they had any level of consciousness they weren’t deep enough for colonoscopy or ERCP, though you could get away with it for a chest tube. “Take him deeper, SP.”
“ I dunno, doc, he’s fkn apneic as he is…”
2. Your post brought back fond memories of Room 5, the chest supplies all grouped together, including the old single-trace ekg machine with the wire and alligator clip to be attached to the pericardiocentesis needle so you knew you ‘were there.’ Checked routinely, used in my presence once.
Thanks, DM.
Divemedic · June 10, 2026 at 12:01 pm
So is arrhythmia. I’m not going to be pedantic.
Conscious sedation, for those who don’t know, is also called procedural sedation. We administer medication to induce unconsciousness without affecting breathing or other life sustaining functions. We use Ketamine, Versed, or Propofol usually. Since there is a risk of overdoing it, it must be carefully monitored through end tidal CO2 and constant monitoring of the patient to ensure we keep them at a moderate sedation level. We keep them under for the 10-30 minutes for whatever we are doing, and then allow them to wake up. The patient is monitored throughout the procedure until 15 minutes after regaining full consciousness. Vitals and sedation level are recorded every 5 minutes while they are being monitored.
The danger of too deep is airway and BP management. The idea is to avoid having to intubate.
No matter what, that is a lot of work for a single nurse to do.
In a large ED, I would wind up assisting with chest tube insertion several times a year. If I were in a trauma center, it would be far more often. Where I work now, I would be surprised if we did it more than once every 2 or 3 years.
Conscious sedation is something I do regularly, perhaps every month or two. I try to avoid it if I can- a risk to the patient, and lots of work for me. So I use workarounds like the ice trick I used last week.
Chris in Nanuet · June 12, 2026 at 6:59 pm
Your content is greatly appreciated. Thank you for taking the time to enrich us.