The President is proposing to court martial and dishonorably discharge any service members who refuse the jab. A dishonorable discharge is a felony conviction.
COVID
Vaccines are racist
If you will remember, if the outcome of anything affects black people more than white people, it is racist. With that in mind, I post this graphic from the CDC for your consideration:
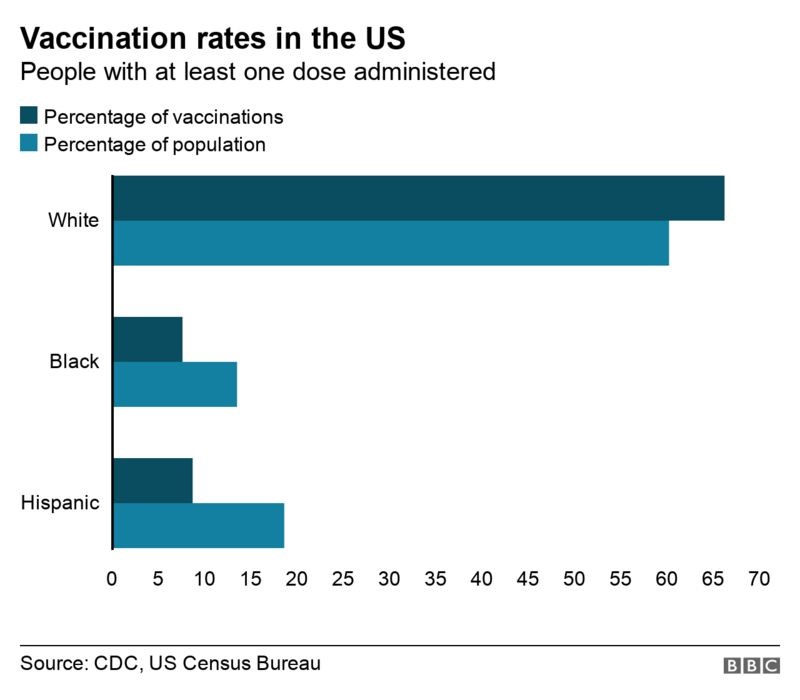
- 65% of vaccinations to whites, only about 7 percent to blacks.
- 15 percent of the black population vaccinated, more than 60 percent of whites.
That, according to their definition, is racist.
COVID
Chloroquine and biowarfare
During the Vietnam war, the US Army had all soldiers who were in country take pills to prevent malaria. The Platoon Medic, referred to as “HOTEL”, came around every morning handing out a “little white pill” that soldiers called the “daily-daily,” and once a week he handed out a big orange pill.
That weekly orange pill contained chloroquine phosphate, 500 mg (equivalent to 300 mg of chloroquine), and primaquine phosphate, 79 mg (equivalent to 45 mg of primaquine). The combination of chloroquine and primaquine has proved much more effective—100% effective in servicemen who took the pill regularly—than chloroquine alone for the prevention of malaria due to Plasmodium vivax. However, it had no prophylactic value for malaria due to P falciparum in Southeast Asia. Therefore, those servicemen stationed in Vietnam, where falciparum malaria is endemic, took a daily dose of dapsone, 25 mg, (the daily-daily) in addition to the chloroquine-primaquine pill. It is approved by the FDA for that use.
How does it work? Chloroquine interferes with the degradation of hemoglobin by lysosomes in a malarial infection caused by P. vivax. One of the things that COVID does is degrade hemoglobin. The release of iron caused by hemoglobin destruction is what damages the lungs. This is why it makes complete sense to me that chloroquine containing drugs would be helpful in preventing hemoglobin destruction and high blood iron.
This also explains why COVID patients have such low blood oxygen saturation, and also why some patients with high saturations are having poor outcomes. The hemoglobin that is there is fully saturated, but since so much of it has been destroyed, the red blood cells simply can’t carry enough oxygen to meet metabolic demands.
Reading the study found here makes me realize that there are a large number of problems and target cells for COVID. I am convinced that this is a biological warfare weapon.
COVID
Too convenient
COVID is killing an average of 0.83 percent of the people who catch it. So why are we hearing about families with 6 dead in 3 weeks? The odds against this are astronomical.
This smells.
COVID
This week’s COVID update
A couple of things. The cases at the hospital are declining. One of the four hallways that we staffed to handle COVID patients was closed this week because our number of patients fell.
The second, and more interesting to me, piece of information came to me last night. I was having a couple of beers with a some military pilot friends of mine. They were telling me the story of the mandated vaccine. The President declared that, since the Pfizer vaccine was now approved by the FDA, he was mandating that all military members get the vaccine.
The military, being the efficient government agency it is, doesn’t have enough of the Pfizer vaccine for the military to get vaccinated. So they solved it by forcing the military to get the Moderna vaccine. You know, the one that isn’t approved.
COVID
Biden cutting off COVID medication to southern states
The Biden Administration, through the Federal Department of Health and Human Services, has cut off the shipment of monoclonal antibodies to Texas, Florida, Mississippi, Tennessee, Georgia, Louisiana and Alabama because of a claimed shortage. The federal government and mainstream media are promoting the restriction as “staving off shortages” due to “dwindling supplies.”
However, you will note that all seven of the states have Republican governors. One of those, Florida, is the governor that Biden threatened just last week. If you remember, he made the statement:
If they’ll not help, if these governors won’t help us beat the pandemic, I’ll use my power as president to get them out of the way.
Make no mistake, Joe Biden and the rest of his administration is at war with the citizens of this country. This decision WILL kill people. This is every bit as despicable as providing small pox infected blankets. This is a deliberate attack against the citizens of the southern US.
If it’s administered within ten days of the initial infection, the treatment can reduce the need to hospitalize a COVID patient by 70 percent, according to medical experts. Governor Desantis has been recommending the treatment since August. My mother and brother both received the treatment and recovered fully with only minor symptoms.
Now the President is using medicine to conduct biological warfare against the south. The first civil war started over much less.
COVID
Let’s do some science
The goalposts keep moving. The latest we are being told is that the COVID vaccine keeps the illness from being as severe. We are told that we should trust the science, and I am a facts and figures kind of guy, so let’s do just that.
So we will do what is called a retrospective analysis of COVID data to see if the presence of the vaccine changed the Case Fatality Rate (CFR) of COVID. All figures for this analysis were obtained from this website.
By December 15, 2020, exactly zero percent of the US population had received a COVID vaccine. Also on that date, 17,299,965 Americans had been determined by various tests to have COVID. Of them, 320,309 had died. That means that 1.85 percent CFR.
In the ensuing months, 70 percent of the public received a COVID vaccine between December and September. So how did it do?
As of September 11, 2021, a total of 41,905,818 had tested positive for COVID. As of that same day, 678,866 of them had died. That means that 24,605,853 people tested positive for COVID and of those, 358,557 died from December 16, 2020 to September 11, 2021. That means a 1.46 percent CFR .
Reducing the CFR from 1.85 to 1.46 represents a 31 percent reduction in the CFR. So what caused this reduction in the fatality rate? There are a couple of things that this could point to:
- The vaccine does in fact reduce the severity of COVID.
- During the first few months of the pandemic, tests were in short supply. For this reason, the only people being tested were those who were the sickest with apparent COVID symptoms. Those who had only mild symptoms, or no symptoms, simply weren’t tested, and this skews the CFR higher.
- The medical profession has simply gotten better at treating the illness.
- The new strains of COVID are less virulent
In science, you want to eliminate all of the variables except for the variable you want to test (called the independent variable) and the result (called the dependent variable). So how do we do that?
The independent variable is the vaccine. We will isolate that by looking at the 90 day period from June 15 to September 15. During that period, an average of 60 percent of Americans was vaccinated.
To isolate the dependent variable, we will look at a 90 day period immediately prior to the vaccine becoming available. That will eliminate factors 2 and most of 3, which will allow us to examine as pure a set of variables as possible with the dataset we have.
So- let’s do some math. From September 15 to December 15, 2020, a total of 10,343,397 Americans tested positive for COVID. During that same time period, 115,703 died. The CFR for the 90 day period immediately preceding vaccine distribution was 1.12 percent. Now from June 11 to September 11, 2021, a total of 7,697,685 people tested positive, and 63,589 died, for a CFR of 0.83 percent. So there was a 25.9 percent reduction in the CFR between the two time periods.
The conclusion here is that vaccinating approximately 60 percent of the public corelated with an approximate 26 percent decline in the CFR. Note that this does not mean that the vaccine was the cause of this decline. In fact, it implies the opposite. If the vaccine were the cause of this decline, the decline in the CFR should have been larger.
Real scientists would be looking into other reasons for the decline. I am betting that they aren’t.
COVID
COVID
A brand new study says that “almost half of those hospitalized with COVID-19 have mild or asymptomatic cases.” Yes, I agree. This is my experience at my hospital.
I think the reason for this is that the hospital tests every single patient who is admitted for COVID, even if they come in for something that is not related to the disease in any way. More than half of the patients in my hospital are COVID positive, but only about ten percent are severe cases, and another ten percent are moderate cases. The remainder- about 8o percent of them, are mild or asymptomatic.
Anecdote: When my nephew and his girlfriend went to the hospital so she could give birth to my grand-niece, they were both tested. Both were COVID positive, but asymptomatic.
COVID
More equal than others
So the workers of the US Postal Service are exempt from Biden’s mandatory vaccine requirement. Can’t be pissing off the people who are redirecting your fraudulent ballots.
This entire thing is an outrage, but let’s keep things in perspective. We haven’t even begun to see how bad things will get. Things are going to get worse. A lot worse, and that is even before the killing starts.