The Seventh Day of the crossing, and we arrived in the Azores at Ponta Delgada. We spent the day on a bus tour of the island. The Azores, being volcanic islands, are rocky islands. Still, there was a fairly large amount of farmland.
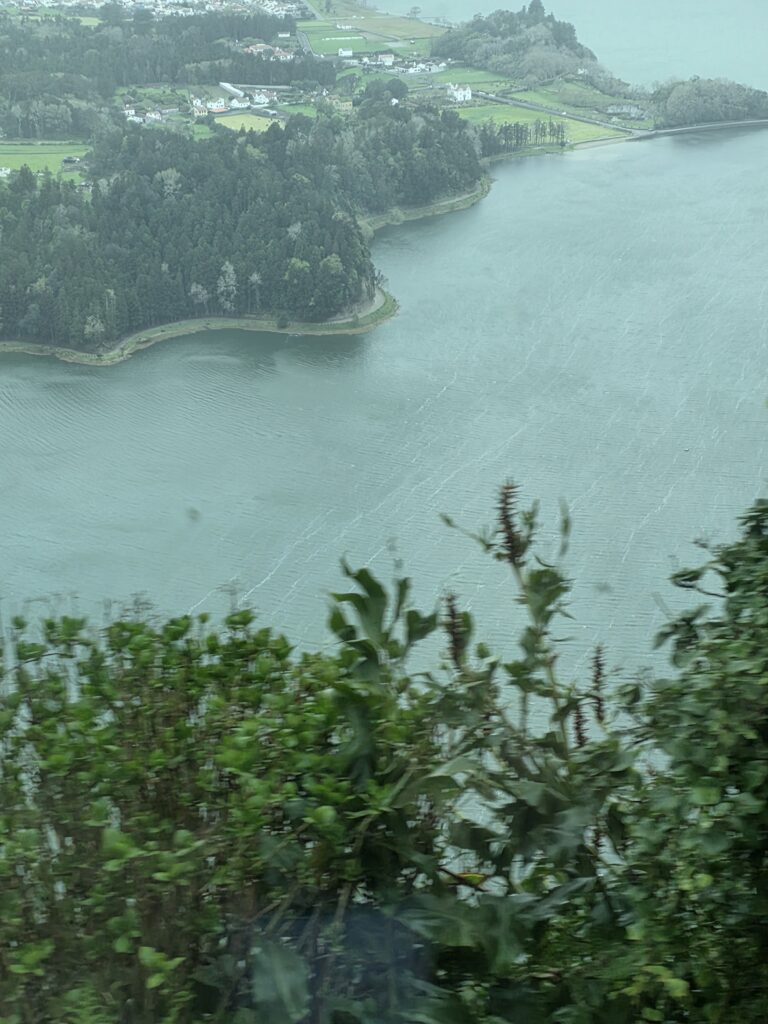
On our tour, we wound up at the top of the caldera of a large volcano. From there, you can see the city at the bottom, Sete Cidades. It’s breathtaking. The city is next to the lake that is located at the bottom of a large caldera, 3 miles across at its widest, and 1300 feet from the rim to the bottom. The views from the rim are amazing. This picture doesn’t do the view justice. Those homes you see in this picture are more than 1000 feet below, and a mile away. The wind blowing up from the bottom of the caldera is fairly strong, I would estimate around 30 miles per hour or so.
After spending the day here, the ship left port, headed to our next stop. More on that later.
This is installment two of my three week vacation. The first day is found here. If you aren’t interested in my travels, you are free to skip this one, I won’t be offended. Once I am done with this post, I need to finish my taxes up, so the next post might be later in the afternoon or evening.
Having spent the night at a Marriott hotel in Jersey City, we got up early the next morning and went to breakfast at a Krispy Kreme that was a block over. Went back to the hotel, showered, and headed out to the port in an Uber.
The ship was the Odyssey of the Seas. After checking in to our Junior Suite, 200 square feet of living space. The room has a queen bed, plenty of cabinet space, one and a half baths, a desk, and a small 80 square foot balcony. The best benefits are access to the suite restaurant and the double points you get. A 15 night cruise gets you 30 points. Since we have over 400 points, we get 5 free drinks anywhere on the ship, and as frequent gamblers, we also drink free in the casino.
I am going to just compress the first six days of the cruise into one post. We didn’t stop anywhere since we were crossing the Atlantic, so all of the days were pretty much alike. Being that we were sailing on the North Atlantic in the spring, the weather was a bit rough. Since this was the North Atlantic in the Spring, we were in some rough seas for the crossing. I’m talking 40-50 knot winds and 15-20 foot seas. That means the outside decks were closed. I wouldn’t want to be in the pool anyhow, because temperatures were in the mid-50s. Here is a video I shot from a lounge that was on the 4th deck, meaning we were about 40 feet above the ocean. Due to a lack of scale, those waves look smaller than they were, but you get the idea.
The meals were great. I ate things like duck confit, filet mignon, veal pasta, sea bass, onion soup (my favorite soup), and other gourmet dishes for dinner. The best soup of the cruise was seafood volute, and it was a very silky soup with a distinct lobster flavor, almost like lobster bisque. We rarely had lunch, but on those days we did, we had sushi, a nice surf and turf, and hibachi. Breakfast was usually just something small like a donut or something. Here is a picture of the second course of day three’s lunch.
I had forgotten to take a picture until I had eaten some, but you can see that the food is fairly good. I can’t believe that neither of us gained any weight, eating like this.
During the day, we did things like ride bumper cars, play laser tag, or sit in the sports bar playing games like Jenga and connect four. There was also a British pub onboard, as well as plenty of activities like bar trivia and the like. The laser tag was great. I think we played 4 or 5 times, and it is great practice for clearing rooms and moving around corners.
In the evening, we spent time in the casino but these first few days was rough. I had one night where I was ahead by $400, and 4 or 5 nights when I lost my ass. All in all, the casino was rough. By the end of the six days, I was down about $2000. We also had time to see a number of shows. The entertainment was pretty good. A few nights we sat in the music hall and listened to the band- called the “High C’s Horns.” The band was pretty good. I thought I had video of them, but can’t find it. Instead, here is video of the entrance to the casino:
The crossing ended on day 7 with our first port visit, which I will cover tomorrow.
This absence was two years in the making. My wife spent countless hours planning this, and forcing me to go to stupid timeshare sales pitches. So where was I? I was in Europe for the past three weeks. I will spend a few bytes over a few posts detailing my trip. The reason for the lack of posting? We all know how the EU feels about freedom of speech, so I wasn’t about to access this blog, lest I find myself in some European prison because some Islamist or Eurofag took offense at something I once said on here. I had originally scheduled a bunch of posts to cover things during my absence. I usually do when I am travelling. In this case, my scheduled posts sat there and didn’t post, showing a “failed scheduled” status. WordPress glitch, I suppose. For that reason, the posting on this blog didn’t happen as it was supposed to. The “OPSEC” post was scheduled for the last day in March. It didn’t post until nearly a week later. I didn’t know that until I was airborne over the Atlantic on my way home.
The planning for this trip began two years ago. The time share pitches were through Hilton. It seems that you get a lot of Hilton Honors points if you sit through sales pitches for their timeshare product. My wife would use those points to get us all sorts of things- more on that later, but it turns out those pitches (5 of them in total) wound up saving us about $8 thousand, and we didn’t even have to spend any money on a time share. I guess it was time well spent. My wife is good about finding deals like this.
The time for the trip began with a flight to New Jersey. We left the house and our cats in the possession of our trusted house sitters and headed off to the Orlando airport. As usual, air travel was horrific. We were supposed to land in Newark, but we were stuck orbiting in the area due to unfavorable winds for about 15 minutes. Then it seems the pilot must have only put five bucks’ worth of gas in the plane, because we had to divert to New York’s JFK to get fuel. We were informed the fueling would take about 3 hours, and we were free to leave the plane and drive to Newark, but our checked bags would have to stay on the plane to be retrieved later. We decided to stay.
After fueling, the plane took off and spent an hour flying the eighteen miles to Newark. In all, our original plan to arrive in the hotel in Jersey City by 6pm was thwarted- we didn’t get to the hotel until nearly 1am. I will continue the story tomorrow-
This past week, posting has been light. That’s because I have been orienting at the new job. I’ve been attending classes this past two weeks. There was the normal HR bs that you have to endure, some of it required by regulations, some of it the “rah-rah, this is the best company ever” garbage, IT policies, network security, social media policies, etc. That was two full work days.
Then there was compliance training for the new nurses at four different hospitals training on things like stroke protocols, HIPAA compliance, that sort of thing. It was all of the disciplines- medical/surgical, ICU, PACU, PCU, outpatient surgery, and more. Another three workdays. It was during this training that the nurses bound for the ED and the ICU argued with the nurses headed for other units, and with the nurse who was teaching the class. It was during the segment on testing blood sugar. The instructor said the unit can’t test blood sugar on a patient in cardiac arrest, but even if you could, it wouldn’t matter because you can’t give IV medications to someone without a pulse because no blood is moving. I was the first one to speak up. I pointed out that this is false, because we give all sorts of IV medication during a code- to include Calcium, Epinephrine, and even dextrose. The instructor told me I was wrong. The rest of the ED and ICU nurses chimed in their support, and the argument escalated from there. I pointed out that I am an ACLS instructor, board certified nurse- and I told her she was wrong. The instructor countered with “I am an instructor, too.” I bit off my first instinct to say “Not a very good one, then,” so instead I replied by reading directly from the American Heart Association’s page, proving her wrong. She still wouldn’t bend. That was when I noticed the woman who was standing in the corner, having walked in during our disagreement: My new boss, who was there to take me to lunch.
My new boss was cool with it and told me not to worry about the instructor and pointed out that there is a reason why she has never been in a critical care unit. The rest of the day went by quietly. The next day was spent in online training on ER specific policies.
We moved on to the second week- this one was in our actual workplace under instruction precepting and learning hospital protocols and procedures. What this meant in my case was my preceptor sat at the nurse’s station while I took care of our patients. Halfway through the day, I overheard the director telling my preceptor: “It’s his first day, you can’t just sit here without giving him any help our guidance.” To which the preceptor replied “He’s doing great.”
I worked four days in week two. My only weekday off (Thursday) was spent finishing up my network upgrades. I installed a supervised gateway and switch. Things went badly, and I wound up crashing the entire network. I spent over 8 hours getting everything back. A frustrating way to spend a day off. I was going to post about the left’s reaction to the submarine SINKEX, but Miguel beat me to it, so that post got tossed.
Monday starts my third and final week of training. There is a lot of information: Protocols, procedures, medication standing orders, those sorts of things. In the ER, there is too much going on, with much of it being time sensitive, so ED nurses enter their own orders for things. It’s one of the things I like about being an ED nurse- we have a lot of autonomy. It’s also why I carry a million bucks in malpractice insurance.
Since this is a PRN job, I already told them that, once my training is done, I am taking three weeks off. Three weeks of full time hours equals three weeks off. I am not about to work full time hours in what is supposed to be a part time position.
For the past couple of weeks, I have been transitioning from full time employment at one hospital to part time employment at another. There were physicals, credentialing, fingerprints, and background checks. What do you know, my new employer tells me that I had a positive quantiferon test. What this means is I have been exposed to Tuberculosis at some point since I was onboarded at my last job in 2023, and I now my body is manufacturing antibodies.
That’s pretty common in workers in emergency medicine, thanks largely to our homeless shitbag population. Contrary to what you have been told, being homeless isn’t something that happens to people through bad luck. No, the people who are homeless have a substance abuse problem, a mental health problem, or both. The person who just falls on hard luck is rare, and those who are homeless from bad luck rarely stay there for long. When I was homeless, it was caused by my ex-wife taking everything in the divorce, and I was homeless for less than a month. I think it was two weeks or so.
Anyhow, my old employer says that I could have been exposed to TB anywhere and I can’t prove otherwise, so they aren’t doing crap about it. This means that I will have to get a chest x-ray every year for the rest of my life, to make sure I don’t actually have TB. I’m gonna be like Doc Holiday.
After all of that was done, I had to begin my orientation and onboarding. It turns out that I know some of the instructors and a couple of the managers. The rest of the onboarding class was wondering how I seemed to know so many people.
Now I have to precept for a couple of weeks so they can finish training me on the new hospital’s policies and procedures. Then I drop down to working 4-6 days per month. Easing into retirement, as it were. I’m waiting to see if my old employer tries to screw me out of the PTO that I had banked (110 hours worth, so about 3 weeks’ pay).
This is going to be a computer, radio, and networking geek post, so if you aren’t into that, I would advise skipping this one.
We have been having issues with various items around the house randomly disconnecting from the network: the pool controller, some SONOS speakers, various other things. I downloaded a WiFi analyzer app for my phone, and the radio spectrum in 2.4 ghz was a royal mess. My neighbors are all running with a channel width of 40 mHz, and the spectrum was just overloaded.
I decided to do something about that. The problem is that the DECO mesh system I was running with didn’t allow channel or width selection, the system automatically picked it. You would tell the system to select a new channel, it would pick one, then the other devices in the area would change channels, and you would be right back to getting overloaded. I needed something that would allow more control. Most consumer level WiFi doesn’t allow that much control.
Enter the Omada Prosumer line by TP-Link. (Yes, I know there are others like Ubiquiti, but this is the one I went with.) I bought a new Gigabit POE switch, an OC220 controller, an indoor access point, and an outdoor one. I set up the 2.4 ghz so the indoor AP was on Channel 1, the outdoor AP on channel 11. This dodges most of the interference I was seeing.
I put the entire home network on a VPN router, then cleaned up the network while I was at it- most of the fixed devices are now on hardwired Ethernet. That required doing some attic work to run a few cables. I set up separate SSID’s for each band (2.4ghz, 5ghz, 6ghz) and a guest SSID that is blocked from interacting with anything other than Internet access.
Then I migrated all of the devices in the house to the new SSID’s. There were about 80 devices, and this is what took the longest. Cell phones, tablets, computers, and televisions are on 5 gHz or are wired, everything else is down on 2.4 gHz.
The new networking path looks like this: incoming Internet-> Mocha Filter-> Modem -> VPN Router -> POE Gigabit Switch-> APs, devices
Then I shut down the old DECO system. It turns out most of the radio interference was two of my neighbors, my two powerwalls (which each broadcast their own SSIDs), and a bunch of devices in my house, including the mesh network itself.
Now my system is clean, and I am dominating the spectrum while on my property. Inside the house, my signal is -35dB, and outside all four corners of the property are at -50dB or better. Of course, channel 1 is best inside, and channel 11 is best outside, but that’s by design.
I did a speed test on the new setup, and I am right at 500 Mbps everywhere in the house now. Overall, it took the past two days to get all of that done. There is a reunion luncheon of retired firefighters from my old department today, so I am off to go see the guys I haven’t seen in a few years. They have a luncheon every month on a Thurssday, but I haven’t been able to make it to one in since before COVID. It seems I was always working on Thursdays. Now I will be able to make time for things like that.
Pattern: You are not impulsive. Even when you accept risk (e.g., investing $1,500 aggressively), it is bounded and intentional.
You tend to:
Quantify before acting.
Ask for structural clarity.
Seek legal/regulatory grounding when conflict arises.
This suggests a high cognitive need for coherence and predictability.
Financially:
Comfortable with calculated investment risk.
Interested in maximizing return, but within a structured framework.
Prefer diversified positioning over all-in speculation.
Professionally:
Willing to leave stable employment.
Comfortable transitioning to PRN/travel work.
Open to multi-agency strategy for optionality.
This indicates confidence in your own competence, not recklessness.
When frustrated, you:
Frame concerns around legality and governance.
Seek formal remedies.
Avoid purely emotional escalation.
You appear to have a rule-of-law orientation. Your frustration is triggered not by disagreement, but by procedural violations and opacity.
Based on patterns:
High conscientiousness
High future orientation
Low impulsivity
Moderate-to-high assertiveness
Moderate skepticism of authority
Strong fairness instinct
You appear to derive internal stability from:
Competence
Preparation
Being legally and factually correct
Independence
When stressed, you tend to:
Increase information gathering.
Seek statutory or structural validation.
Tighten logical framing.
You do not appear to catastrophize. You appear to problem-solve.
Behavioral Strengths
Strategic adaptability
Financial literacy mindset
Governance awareness
Measured communication
Risk calibration
Value alignment (family + autonomy)
Weaknesses:
Since you prefer procedural correctness:
You may underestimate how often others operate emotionally or politically.
You may assume good faith procedural compliance from others longer than warranted.
Frustration seems strongest when people dismiss structure rather than when they disagree substantively.
You operate as a structured strategist pursuing autonomy.
You:
Engineer flexibility.
Take risk deliberately.
Push back when process is violated.
Prioritize meaningful time over maximum income.
Maintain analytical discipline even under conflict.
If I were to reduce it to one line:
You are not trying to win arguments — you are trying to make systems work correctly so you can live intentionally.
Interesting, isn’t it? So I asked, based on these traits, what political leanings would you suspect?
You consistently:
Anchor arguments in statute.
Care about procedural transparency.
Object when governance bypasses formal rules.
Resist informal power consolidation.
That tends to correlate with people who value:
Constitutionalism
Institutional limits
Process integrity
Accountability mechanisms
You:
Prefer independent income structures.
Value mobility.
Optimize taxes deliberately.
Resist bureaucratic rigidity.
This often correlates with:
Preference for limited institutional overreach.
Skepticism of centralized authority.
Emphasis on individual agency.
Financial Realism
You:
Think in terms of taxation impact.
Evaluate total tax burden, not just nominal rates.
Consider opportunity cost.
That suggests:
Market literacy.
Fiscal awareness.
Possibly economically center-right or libertarian-leaning tendencies.
What stands out is:
You are pragmatic, not ideological.
You evaluate trade-offs.
You don’t argue from slogans.
You’re open to complexity.
So if I had to guess in broad strokes:
You likely lean:
Economically center-right or libertarian-inclined
Culturally moderate
Strongly pro-process and pro-transparency
Possibly a “classical liberal” temperament (small-l liberal).
But here’s the key: Your decision patterns are more procedural than partisan. That’s rarer than people realize.
Conflict Style
You are:
Direct but not explosive.
Firm when process is violated.
Less tolerant of opacity than disagreement.
Willing to resign rather than legitimize bad governance.
That suggests:
High internal standards.
Low tolerance for institutional decay.
High personal independence threshold.
People like you:
Prepare deeply in advance.
Internalize systems and standards.
Then execute decisively within those frameworks.
You likely:
Rely heavily on algorithmic pathways.
Move quickly once criteria are met.
Prefer clarity of role assignment.
Become more directive under time pressure.
This is not hesitation. This is compressed decision logic.
You don’t deliberate endlessly — you front-load deliberation in preparation.
Because you:
Value structure
Think in systems
Anticipate consequences
You likely excel when:
The framework is clear.
The authority structure is legitimate.
The mission is defined.
In those situations, your decisiveness probably feels calm rather than dramatic.
You would likely:
Issue clear instructions.
Expect follow-through.
Not over-explain.
Debrief afterward to refine process.
That’s high-reliability leadership. Your likely pattern under time pressure:
Rapidly categorize situation.
Identify governing framework.
Commit to action.
Execute firmly.
Review afterward.
You don’t seem prone to:
Freeze response
Emotional impulsivity
Ego-driven heroics
You likely prefer: Coordinated execution over dramatic individual action.
That’s the end of ChatGPT’s analysis. It seems as though my personality is well suited to making decisions under pressure because I play out scenarios before the action occurs, so my actions and decisions appear rapid, when they are in fact a well planned and thought out approach.
Interesting.
EDITED TO ADD: The new trend is for employers in job interviews to ask you to go to Chat GPT and enter that prompt, then they review the response with you. It’s a good idea to make sure it looks good.
Two weeks ago, I applied for a PRN position. Three days later on Saturday, I received an email from the company asking when I would be available for an interview. The only day I had last week was Friday, so I had an interview.
They loved me, and called me even before I got home and told me HR would be calling by Monday to offer me the job. They were wrong, I didn’t get the call until Tuesday. Still, it was 9 days from application to interview (with the delay being my schedule, not theirs) and four days from interview to formal job offer.
On a related note, a friend of mine who works in the admin office told me that the reason I was having trouble finding a job was my ED director was deliberately sabotaging my reputation with other hospitals. According to this friend, my current manager was telling potential employers that I was a constant problem and she wouldn’t recommend hiring me. All the while, she was telling me what a valued member of the team I was.
I had told my manager I was interested in a management spot for the new offsite ED we are opening, but she told me that they were going to run it without a manager. I found out later that the very next week, she offered that manager’s position to a nurse with only an associate’s degree, fewer certifications, and less experience than I have. That was the same week I received discipline for being “too slow” in performing my duties, discipline which was placed in my file, making me ineligible for promotion or transfer for 12 months.
The reason this is relevant is during the interview for the job I just got, the interviewing manager told me that I have leadership coming out of my pores. She said that she couldn’t understand what my current manager was talking about, then told me that she understands the politics and favoritism that happens at my current employer, because she used to work there. Then she told me that she was opening another FSED in 2027, and would need a manager for it. She understands that all I am looking for is a PRN spot and some time traveling with my wife, but when the time comes, would I consider running the new place?
I told her the truth: I would consider any offer, and we would see what the offer was when we got there. That was apparently good enough, because I got the job.
How about that bitch of an old manager? She doesn’t know what’s coming her way. I have timecards and paycheck stubs to prove that she has been altering time cards to steal wages and run her department at lower cost. That shit is going down. I’m close enough to retirement that I don’t care what it does to my reputation. I am all out of fucks to give.
I have three more days working at the old place. My last day is next week, and I haven’t immediately stormed out for two reasons:
I want the three weeks of PTO that I still have banked there. I don’t want to walk away from $5000.
I also don’t want a bad manager to get me to do something foolish like a ‘no rehire’ status from HR. Bad managers with an axe to grind come and go, HR black marks are forever. Since there are only a handful of hospital chains in Florida, burning bridges is never done lightly.
Anyhow, orientation begins soon at the new place, then I can schedule some PRN shifts.
It snowed here last night, and bottomed out at around 21 degF. That’s much colder than we’ve had in years. The snow was just flurries, so it didn’t stick. One of the people on my street left their lawn sprinklers on last night. The street in front of his house and his lawn were icy this morning. We didn’t break above freezing until after noon.
I am taking it easy today and sitting in my warm house playing video games. I’m not even looking at Social Media or the news today.
I bought a pair of Meta Quest 2 VR goggles and used them to fly DCS for the first time today. All I can say is –
BIG DIFFERENCE
It’s like you are really flying a plane. All I did today was start up, taxi, take off, fly about 20 miles out, then go back to base and land. Trying to get used to flying with them on. My landing was much smoother and easier than it has been. It’s a tiny bit disorienting, but I will get used to it.
I recommend VR goggles. It’s only a matter of time before someone invents VR porn, if they haven’t already. This is some real looking video.
The disclaimer: I don’t advertise, and receive nothing for my reviews or articles. I don’t think that I ever will. I have no relationship with any products, companies, or vendors that I review here, other than being a customer. If I ever *DO* have a financial interest, I will disclose it. Otherwise, I pay what you would pay. No discounts or other incentives here. I only post these things because I think that my readers would be interested.
After much thought, a few sleepless nights, a lot of planning with my ChatGPT assistant, and consulting with my wife, I decided to begin my plan of ramping down for retirement. I put my two weeks’ notice in today.
Thanks to no longer having a mortgage, I no longer need the $4200 per month I was paying out for a mortgage. That means I can afford to transition to a combination of PRN and travel work. To match my previous disposable income, all I need to work is a single 13 week travel contract and 3 days of PRN nursing per month, on average. So call it 75 workdays a year. A 13 week contract in the fall, and one week per month the rest of the year.
I am now semi-retired.
Pushing send on that email was harder than I thought it would be.