So we are on that message again?
Another study claims that the unvaccinated are more likely to get in serious car accidents. Look for your car insurance to be increased unless you take the vax.
So we are on that message again?
Another study claims that the unvaccinated are more likely to get in serious car accidents. Look for your car insurance to be increased unless you take the vax.
Joe asks in comments if I have heard anything about this article referencing a “tripledemic” of RSV, COVID, and Influenza.
Respiratory syncytial virus, or RSV, is a common respiratory virus. It usually causes mild, cold-like symptoms. RSV usually strikes children before the age of 2, and is also known to have a severe effect on those over 65 and with weakened immune systems. In the United States, nearly all children have been infected with RSV by age two. This virus has a season, and in the United States, Florida and Hawaii’s season begins in mid September, with the rest of the country’s RSV season beginning by mid-November. The incidence of RSV peaks each year by mid-winter. It is an airborne virus that can also be spread by fomites.
A fomite is a surface that is contaminated because a virus that can live for a time outside of its host is on the fomite’s surface. A person touches the fomite and then touches their face. The average person touches their face 4,000 times a day. Kids even more so. This is why frequent handwashing can be effective in preventing illness.
Influenza also has a season, as we all well know. It also strikes the immunocompromised and the elderly.
Until 2020, patterns for RSV in the United States were predictable. The patterns of RSV and other common respiratory illnesses have been messed up since the lockdowns in 2020. The number of RSV infections began to rise in the spring of 2021 and peaked in July. Why? I mean, this is usually a winter virus.
In 2020 and into 2021, there weren’t many cases of seasonal illnesses because kids were largely kept out of school during the peak RSV and flu seasons during the winter of 2020-2021. In most states not named Florida, the same happened during the 2021-2022 season, so all of the kids who would have brought the virus home to their younger siblings weren’t in school to do so. That means all of the kids born in 2019, 2020, and 2021 have not been exposed to RSV and this will create a heavier than usual RSV and flu season. It makes total sense.
The same is true of the flu. This year, the season appears to be starting a bit earlier than usual, but that is not surprising, considering what I discussed above. The past couple of years have been unusually light for the flu, and I think that we are going to have a rebound year.
So what does this mean? Nothing. Most people who get it have a bit of a cold and then soon recover.
As far as COVID: granted that this is anecdotal, but we don’t seem to be seeing any more COVID than we have been seeing for the past year, at least not in my hospital. It’s just a constant background now. I have had it twice, and I don’t even bother to wear a mask when I treat COVID patients any more. The CDC is not really reporting a high number of COVID cases right now.
I don’t think that there is anything to make a big deal out of right now. That may change, but for now I don’t think it’s anything to get in a lather over.
JKB over at gunfreezone asks why medical training requires doctors to do rotations in specialties that are not their own, pointing out that engineers in one field don’t have to also do internships at a civil engineering firm, a mechanical engineering firm, a structural engineering firm, and a chemical engineering firm. He states that it looks like a complete waste of the student’s time. The reason that medicine does that is actually pretty simple, so let me give a simple explanation.
It isn’t likely that a mechanical engineer will do something that will have a direct effect on a chemical engineer’s job. That chemical engineer isn’t likely going to have an issue with avoiding the problems that a structural engineer is having. Imagine if a mechanical engineer tightened a screw a quarter turn, and this caused the hydraulic fluid to become acidic and then the building collapsed. Not so in medicine. Sure, people in medicine tend to specialize, but the human body is a complex system, and changes to one system have profound effects on the others.
Let’s say that I am in cardiology and I have a heart failure patient who is in fluid overload. There are a number of drugs that one could choose from to get rid of those fluids. I could try furosemide, or perhaps bumetanide. Perhaps torsemide, or even hydrochlorothiazide. Any of those medications would likely solve your patient’s issues, but which one of these is going to be detrimental to the patient’s kidneys? Do I want to choose a potassium sparing or a potassium wasting diuretic? How will that react with the patient’s preexisting autoimmune dysfunction? I could consult a nephrologist, an endocrinologist, and an immunologist, but doctors largely don’t stand around most of the time having huge arguments. That only happens on TV shows, not because there are no egos involved, because there are. Medical people are just too pressed for time to keep doing that, so wouldn’t it be easier if I already knew?
So for that reason, most in medicine learns a little about every system and specialty before going on to gain a deep understanding of their specialty. Nurses, doctors, PAs, NPs, all of them.
The first comment on that post complains about sterile fields and how they are “superstition.” Sterile fields are there to prevent post procedure infections. You can’t see infectious agents. Perhaps you didn’t touch anything. Or maybe you bumped into something that was covered in S. aureus and didn’t notice. How do you know? Can you be sure? If you are wrong, you will know in couple of days when your patient goes septic. You can’t bet a patient’s life on “the ten second rule.” Certain behaviors are high risk, so procedures get written in to the process to reduce or eliminate those higher risk behaviors. That includes treating everything that “breaks field” as though it was covered in an infectious agent- because it might be, and there is no way to know for sure. So you toss the offending object aside, and use one that you KNOW is sterile.
As an example, the most common cause of hospital caused infections is a CAUTI (Catheter Associated Urinary Tract Infection). It’s caused by a catheter introducing a pathogen into the urinary tract. That can affect the kidneys. It can cause Acute Kidney Injury. In some cases, that can cause Chronic Kidney Disease and ultimately kidney failure, or it can cause septicemia (a blood infection), which leads to death. Because of this, there are procedures that need to be followed when inserting, caring for, and ordering indwelling catheters. Can you violate that procedure and get away with it? Sure. A few times. Maybe only once. But one thing is sure, you will eventually wind up with a septic patient. So the procedure is there to prevent that.
I am sick of hearing people talk about how this person or that one is spreading misinformation, and how people who do should be silenced, deplatformed, or even jailed, when this is the timeline of COVID vaccines, as told by the MSM:
November of 2020: Moderna said Monday that early analysis from its Phase 3 trial shows its Covid-19 vaccine is 94.5 percent effective at preventing the illness, offering hope of a second breakthrough in as many weeks. The news comes a week after pharmaceutical giant Pfizer said early analysis showed its vaccine candidate was more than 90 percent effective. NBC NEWS (emphasis added by me, in red)
March 4, 2021: Both the Pfizer/BioNTech and Moderna vaccines were primarily evaluated for their ability to prevent symptomatic COVID-19, with the former having a 95% efficacy and the latter having a 94% efficacy in the clinical trial data submitted for the original authorization by the Food and Drug Administration. This means your risk of getting sick is cut by 94% or more if you are vaccinated. The final phase 3 data showed an efficacy of 91% for Pfizer/BioNTech and 93% for Moderna. A quote directly from factcheck.org (emphasis added by me, in red)
April 28, 2021: The Pfizer and Moderna vaccines were 94 percent effective in preventing hospitalization for COVID-19 among people age 65 and older, according to a Centers for Disease Control and Prevention (CDC) study released Wednesday. The Hill.com (emphasis added by me, in red)
March 28, 2022: Three doses of the Pfizer or Moderna vaccines were 94 percent effective in preventing death or the need for a ventilator during the omicron surge, according to a new study. The Hill.com (emphasis added by me, in red)
Note that the goalposts continue to move. At first, it was two doses were 94% effective in preventing the illness, then it was preventing symptoms, then it morphed into preventing hospitalization in people over 65, then it became three doses preventing death or a ventilator.
So who exactly is spreading misinformation? My guess is, everyone. Simply because some people are lying, some don’t know anything, and no one really knows the truth. Well, someone does, but they aren’t telling anyone.
Five days ago, I posted about the hospital where I work trying to save money by cutting out the shift bonuses that were being used to entice the staff to work 50 and 60 hour workweeks. Today was the first day where I worked and there were no overtime people. Where a 50 bed ED normally needs 14 nurses to operate? We had 10 for most of the day. Meaning that we should have 5 patients to each nurse.
Nope, we were too busy for that. We tried to tell EMS agencies that we couldn’t take any more patients (it’s called being “on divert”). It didn’t work. At one point, we had 90 patients. For ten nurses.
I work a swing shift, which is supposed to be 11am to 11pm. Most of the ED works 7-7. By 9pm, my patients were:
For those of you who don’t know, most of those patients need to be in a unit that offers a higher level of acre than what we can provide in the ED. The problem is that all of those units are already full.
In the meantime, there are 22 people in the waiting room, waiting for us to have room to treat them. At one point, there were 7 ambulances lined up at the door, waiting to drop off patients. So I wound up ordering Wendy’s through DoorDash at around 8pm, and eating it at the nurses station while I wrote notes on patient’s charts.
Needless to say, everyone was getting testy, patients AND staff.
As 11 o’clock approached, the charge nurse asked me to hold over because we still had more than 60 patients, and three of us were scheduled to go home at 11, which would leave her with no techs and only 8 nurses. Because I like her and she always does me favors, I agreed to hold over for a couple of hours.
Right at 1, when I was planning to go home, all hell broke loose. An intoxicated woman was brought in by EMS, who claimed they were unable to get an IV. Ten minutes after they dropped her off, she vomited about a 1.5 liters of blood.
So a third of the remaining nurses spent the next 45 minutes trying to keep her alive. All of their patients were getting ignored in the meantime.
One nurse remarked, “As long as we keep doing this, they will keep making us do it, until it becomes the ‘way we have always done things.'”
I finally left the place at around 2 am, having worked a total of 15.5 hours. But think of all the money they are saving by not having to pay those bonuses.
Last month, I mentioned that the hospital where I work is bringing Philippino nurses in to fill vacant positions for less money than hiring Americans. There is more news on that front.
We have been short staffed for nearly three years. They have made up the shortfall by paying huge bonuses to get nurses to work extra shifts. They tried foreign workers. Still, they don’t have enough. Determined to save money now that the COVID funding has dried up, hospital administration announced on Saturday that there will be no more bonuses offered. Once the shifts that are already promised bonuses are paid out, they will be no more. Nurses who were making $2500 a day for working a 12 hour over time shift are now being asked to work the same overtime hours, but for $600-$900 each 12 hour shift.
I know that I was working 60 hours or more a week. I was making good money to do that, but now that the money has dried up, I am not working those kinds of hours for a fraction of the pay. No one that I know is willing to do that.
So now the entire staff of the ED is not taking any extra shifts. They are working their contracted hours, and that is it. Me? My contract says that I have to work 4 shifts a month. That is all I am doing. Everyone else is doing the same. So now the hospital is even more short handed.
Here is what was texted out to us this morning by the ED department head:
Hello team
We know this week has definitely had its ups and downs already and we appreciate all the hard work done by everyone. While we all fight this same battle we still have patients who are expecting the best care we can provide.
Starting tonight through the weekend we could use anyone on any shift to assist your fellow team and patients.
Please any help is appreciated.
As if guilt tripping us will get us to work all of those extra hours for a third of what we were making before. I want to help my patients and coworkers, but at the end of the day, this is a financial arrangement. It’s business.
So now the hospital is getting desperate. A third of the ED beds were shut down today for lack of staff.
The hospital where I work can only fill itself to somewhere near 60% capacity because they don’t have enough nurses, and that was when people were working extra shifts for bonus money. That means that patients often stay in the ED until there is an open bed on the inpatient floors. Our ED is frequently more than half filled with patients on “admission holds” awaiting beds. Couple that with the fact that the ED is also short nurses, and you have a problem.
Picture a 50 bed emergency room. To staff a 50 bed ED takes 14 nurses, 4 paramedics, 4 general technicians, 3 doctors, a nurse practitioner or PA, a respiratory therapist, secretary, three registration clerks, two lab technicians, three radiology techs, and two janitors. Every shift.
Now picture that you only have enough nurses for 10 per shift. Now you can only handle 40 patients at a time instead of 50. Now also picture that you have 30 admit holds, taking up beds and waiting for an inpatient bed- some for more than 48 hours. Now you can only handle 10 patients because your staff is busy caring for holds. So the waiting room backs up.
This means you have people sitting in the waiting room for 4, 5, or even 6 hours as they wait for treatment. And all of that was happening before you cut off the bonus money.
Now instead of 60% staffed, you are more like 45% staffed. Instead of 10 nurses, you only have 7. Now picture that across the entire hospital. A 600 bed hospital with a 50 bed ED requires 100 nurses or more each shift. You only have 50 or 60. Now what do you do? There aren’t enough foreign workers to fill that many spots.
My hospital can’t be alone in this. Here is the warning: there is a potential collapse of health care coming. It takes 3 to 4 years to train a nurse to the point where they are licensed, and another 2 years or so for that nurse to be proficient enough in their job to staff an ED, even longer for places like the ICU.
The CDC finally admits that the vaccines don’t work. Does that mean all of the fact checkers owe people some apologies?
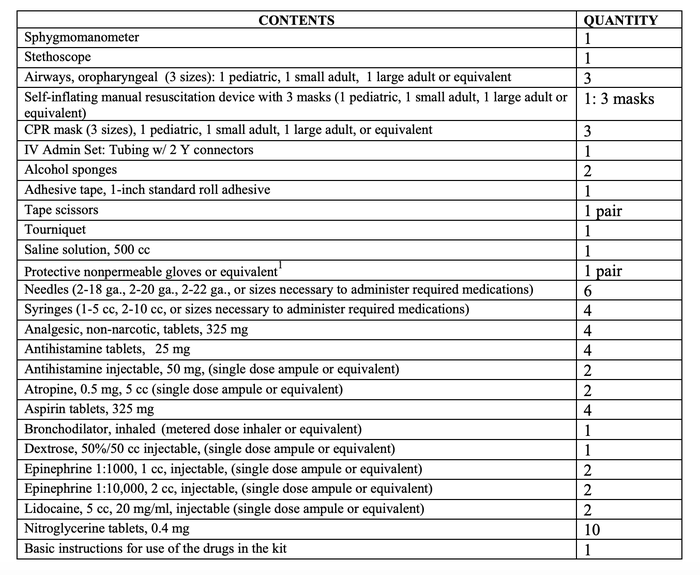
Because of the comments to the post about the doctor on the airplane, I wanted to do a follow up. So let’s first talk about what is in the medical kit on a commercial aircraft. The FAA requires an AED, and a medical kit that contains the following items:
The most common inflight medical events are:
My wife was on an aircraft flying from JFK to Heathrow where there was a death in flight. The flight attendants cleared out the back row of the plane and put the body on the seats, covering him with a blanket. That is where he stayed for the remainder of the flight.
I myself have been on two flights were there were medical issues. In both cases, the flight crew called for medical personnel. I wasn’t going to volunteer, but no one else did, so I raised my hand. The FA brought me a radio headset that was connected to the airline’s on call doctor, who consulted with me and we agreed upon a course of action.
The first was a moderate allergic reaction (urticaria, wheezes, pruritus) on a flight from Orlando to Boston. The passenger got himself 50mg of IV diphenhydramine and some inhaled albuterol. He was fine and slept the rest of the flight.
The second was on a flight from Las Vegas to Orlando. It was a guy who was having himself an anxiety attack. He was hyperventilating and complaining of shortness of breath, chest pain, along with numbness and tingling to his fingers and lips.
The reason for it was hilarious. He had gotten married to his fiancé (a white woman) while in Vegas. He was Puerto Rican, and was dreading his mother’s reaction when he told her that he had married a woman (who wasn’t Puerto Rican) that his mother hadn’t even met yet. If you know anything about Puerto Rican mothers, you would know that they are much like Italian mothers. He had every right to be afraid.
Anyway, I told the doctor that his vitals looked good and I felt like it was an anxiety attack. The doctor agreed. I traded seats with his wife for about half an hour and talked him down. Once he felt better, I went back to my seat. An hour later, his wife came and got me a second time. During that second visit, his wife told mine that I was a very patient and nice man.
That’s it for my aircraft stories.
I don’t feel sorry for this guy.
To the press: stop whitewashing this:
Matt Ford, who goes back and forth between both New York City and Los Angeles, had been exposed via a friend in LA through skin-to-skin contact.
If you don’t want monkeypox, you should stop sticking your penis in the rectums of other, random men.
Elmo from the children’s show “Sesame Street.” got a COVID-19 vaccine Tuesday. Programming kids to be good little communists.