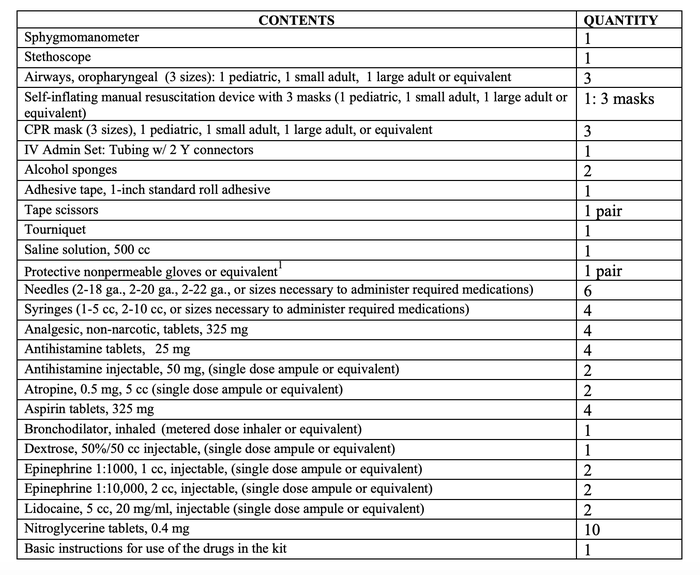
Because of the comments to the post about the doctor on the airplane, I wanted to do a follow up. So let’s first talk about what is in the medical kit on a commercial aircraft. The FAA requires an AED, and a medical kit that contains the following items:
The most common inflight medical events are:
- Gastrointestinal/Nausea (31%)
- Neurological, such as fainting or seizures (26%)
- Respiratory (7%)
- Cardiovascular (5%)
- Dermatological (5%)
My wife was on an aircraft flying from JFK to Heathrow where there was a death in flight. The flight attendants cleared out the back row of the plane and put the body on the seats, covering him with a blanket. That is where he stayed for the remainder of the flight.
I myself have been on two flights were there were medical issues. In both cases, the flight crew called for medical personnel. I wasn’t going to volunteer, but no one else did, so I raised my hand. The FA brought me a radio headset that was connected to the airline’s on call doctor, who consulted with me and we agreed upon a course of action.
The first was a moderate allergic reaction (urticaria, wheezes, pruritus) on a flight from Orlando to Boston. The passenger got himself 50mg of IV diphenhydramine and some inhaled albuterol. He was fine and slept the rest of the flight.
The second was on a flight from Las Vegas to Orlando. It was a guy who was having himself an anxiety attack. He was hyperventilating and complaining of shortness of breath, chest pain, along with numbness and tingling to his fingers and lips.
The reason for it was hilarious. He had gotten married to his fiancé (a white woman) while in Vegas. He was Puerto Rican, and was dreading his mother’s reaction when he told her that he had married a woman (who wasn’t Puerto Rican) that his mother hadn’t even met yet. If you know anything about Puerto Rican mothers, you would know that they are much like Italian mothers. He had every right to be afraid.
Anyway, I told the doctor that his vitals looked good and I felt like it was an anxiety attack. The doctor agreed. I traded seats with his wife for about half an hour and talked him down. Once he felt better, I went back to my seat. An hour later, his wife came and got me a second time. During that second visit, his wife told mine that I was a very patient and nice man.
That’s it for my aircraft stories.



