Trudeau is a groomer. I don’t care what your courts have to say about free speech.
Race baiting
Blacks Want Segregation
Former NFL player Rashard Mendenhall says that:
I’m sick of average white guys commenting on football. Y’all not even good at football. Can we please replace the Pro Bowl with an All-Black vs. All-White bowl so these cats can stop trying to teach me who’s good at football. I’m better than ur goat.

Remember the time that Rush Limbaugh wanted to buy an NFL team, but the players union stated that they would refuse to play for him, so he got rejected? The reason he was rejected was for a statement like this:
The NFL all-too-often looks like a game between the Bloods and the Crips without any weapons.
There are those in the sports commentator ranks who have no problem attacking their own race to get their valid left wing street cred.
Rush still lived on to launch Donald Trump and put his permanent stamp on the Republican Party as one rooted in white grievance, bigotry, and incitement to violence.
This is the same attitude that saw football players taking a knee and calling the NFL the slave plantation. I’m over all of this. It’s time that the blacks of this nation stop appropriating white culture. We invented football. Let the Africans play African sports. What sport did they invent again?
Let them live in houses that were invented by Africans. They would all live in mud huts. Sub-Sahara African negroes have invented nothing: farming, building construction, sanitation, and sports are all beyond their capabilities. Art? African art looks like a preschooler’s Pla-Do sculpture of people screwing.
So let’s just agree to let blacks have their culture. What is their culture again? They can’t even do drive-by shootings and sell cocaine. Both of those were invented by whites as well. At least they will have ghetto apples, live in mud huts, and eat fried chicken. Oops, fried chicken was invented by whites as well. Holy shit, what did they invent again?
Still, I am at a point where I fully support Mendenhall’s position. It’s time that we segregate the black race from white society. Let the US negro have their own state. All of them can move there and live their lives steeped in their culture. No more welfare, jobs, food, or banking. Go. I can live without all of the things that blacks bring to the table: shootings, drug abuse, violence, and that horrible rap music. We will even let you have the NBA, even though you won’t have any money to pay your players because your fans won’t have money to buy tickets without EBT cards.
Stereotypes suck, don’t they?

Grooming Children
Grooming
The following poster was seen in a high school. When you first go to their website, you are told by a popup how to hide the fact that you are on their site. That’s because GLSEN is a secret teacher organization whose aim is to turn kids into good little leftist faggots. They are deliberately grooming your kids.
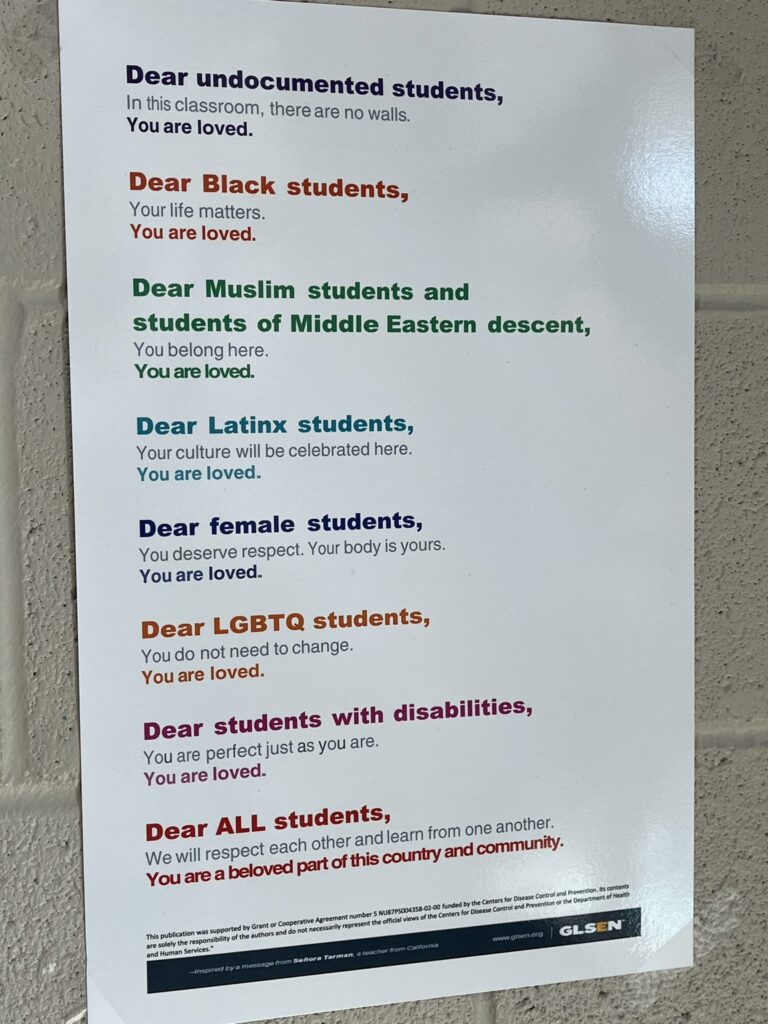
Read the bottom. It was paid for by a grant from the CDC to GLSEN. How is printing things like this even remotely connected to the CDC?
Take another look at the content. Women, Fags, Illegal Immigrants, Hispanics, Arabs, and the disabled. Do you see what’s missing? Yeah, straight white males. Remember back in the 80s, when it was illegal to charge extra for accepting credit cards, so businesses gave discounts for using cash?
This is the same concept. They can’t discriminate against whites without backlash, so instead, they are giving special privileges to everyone EXCEPT straight white males. They get privileges that YOU paid for, and you get nothing but the bill. Even Time magazine says that you are the enemy because all white people are racist oppressors.
This is how the US military turns on white neighborhoods. Remember that currently, only 45% of the US military is white men. A number of those white men are fags and trannies. So call about 40% of the military is straight white men. The airstrikes, door kicking, and missile strikes will be OK, because it will be against their racist white oppressors.
Uncategorized
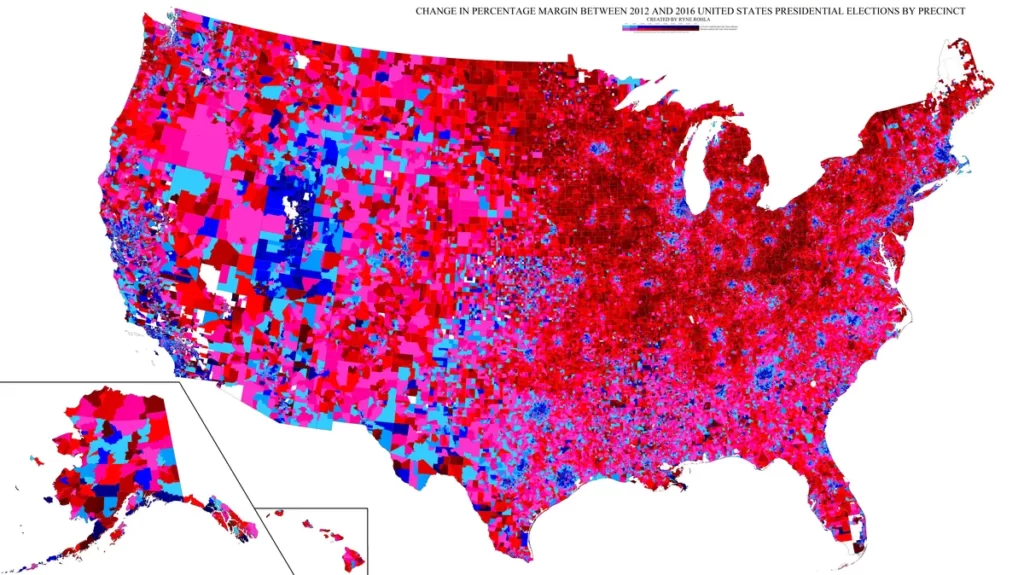
Battle Lines
Here is a precinct level map of the 2020 election. This is where the battle lines will be.
Presidency
First Domino?
Now that the Colorado Supreme Court has disqualified Trump from holding any public office, will this be the first domino? Are we seeing the first steps towards the 2024 cheat? Is this the next step in an American dictatorship?
Here is the tracker. This is important. Colorado is out of play for Trump, meaning that even if he DOES get the Republican nomination, he has just lost 10 electoral votes. Now Biden doesn’t have to cheat or even run for office in that state. He is the default winner. Watch this closely. If only ten states disqualify Trump, there is no point in even having the election. It’s a done deal.
The Republicans have no balls. If they did, Colorado delegates would not be seated at the convention.
It’s a good thing that the Democrats saved our Democracy, eh?
Illegals
Are We Being Overrun?
The State of Minnesota has selected a new state flag. Here it is.

Now compare that to Jubaland, state of Somalia flag.
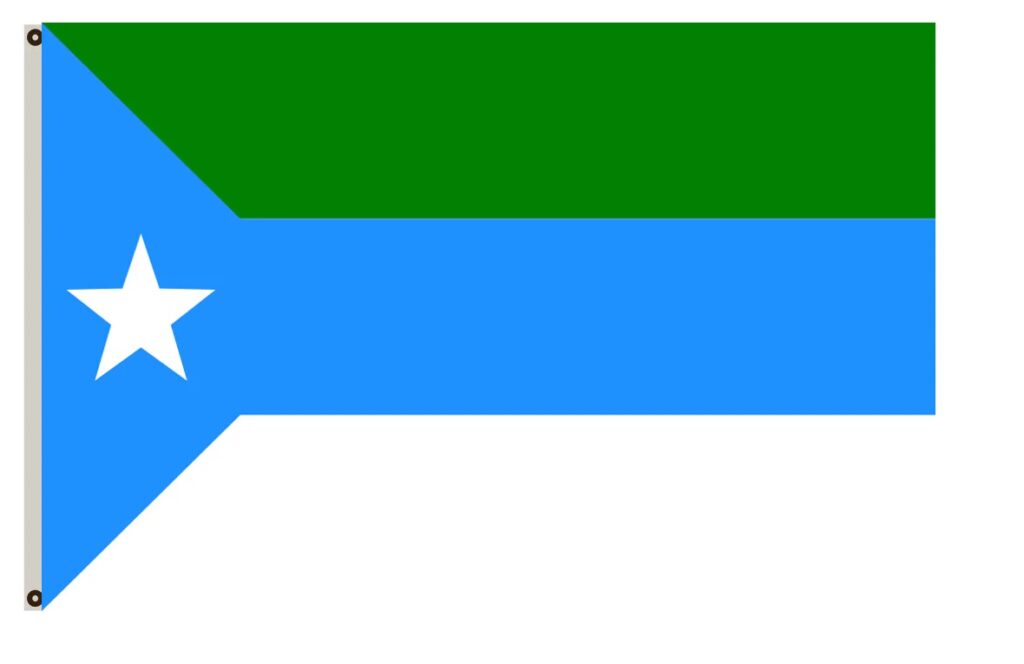
Look kind of similar, no? Hey, it’s no worse than Canadians singing their national anthem in Punjabi.
Uncategorized
NY Proposes Law to Force Chik fil A to open on Sunday
New York is proposing a law that would require fast food establishments located in state highway rest stops be open seven days a week, a move that they admit is aimed at the Christian restaurant chain.
Police State
Lawfare
Now it isn’t just Trump. The Biden administration is using Federal Law enforcement as a weapon against Florida’s Governor DeSantis.
This is the mark of a dictatorship- having your opponents jailed on bogus charges.
Military
Third World
As I have posted before, the US military will obey orders to attack Americans. The only good news here is that this is what the US Army is becoming:
That’s why they are begging the guys who were kicked out for failing to get the jab to return. The left thinks that having guns is all that is required to win. It isn’t just the possession of guns, it’s the will and the knowledge to use them, as well as the ability and determination to do whatever it takes. A bunch of barracks soldiers who won’t do their jobs isn’t going to be up to the task.
This is a third world type of military, one which is only good enough for intimidating and massacring a bunch of unarmed civilians. They surely will have a hard time beating an armed and determined foe.